A 40 yo patient presents with a complaint of total arm paraesthesia and global loss of power. Over 16 hours previously she had a surgical procedure on her hand. A Brachial Plexus block (axillary approach), was used to provide anaesthesia. There has not been any return of function.
 On examination there is a total loss of sensation to the arm, loss of grip strength and a wrist drop.
On examination there is a total loss of sensation to the arm, loss of grip strength and a wrist drop.
Management of this patient?
 A rapid bedside ultrasound was performed that demonstrated a collection. A formal ultrasound then demonstrated a haematoma of 15mm x 140cm surrounding the axillary-brachial plexus complex.
A rapid bedside ultrasound was performed that demonstrated a collection. A formal ultrasound then demonstrated a haematoma of 15mm x 140cm surrounding the axillary-brachial plexus complex.
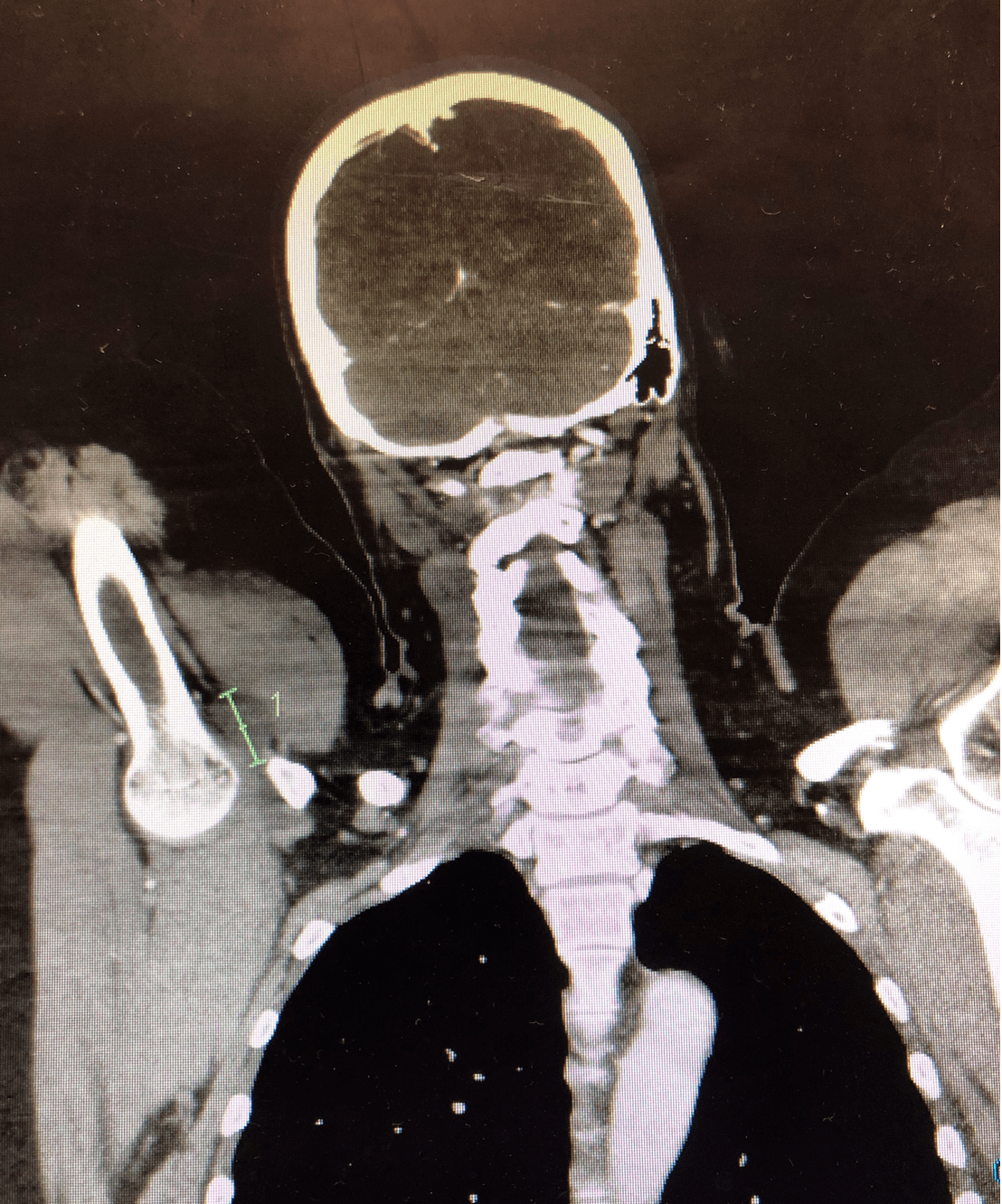
Given no MRI was available, a CT was performed by the surgical team that was not as clear. It potentially also showed some nerve oedema.
The patient was transferred to a Quaternary centre for combined vascular and neurosurgical operative intervention.
What is a Brachial Plexus Block?
It is a technique for establishing operative anaesthesia and pain relief of the upper limb.
There are three main approaches, each with a different potential complication.
- Interscalene approach: It is indicated for procedures on the shoulder and proximal humerus It can be used in surgery of the arm or forearm, however there is a high incidence of incomplete inferior trunk blockade, such that the ulnar distribution, is inadequately anaesthetised. It is associated with a higher incidence of dysfunction including potential injuries of the spinal cord and vertebral artery puncture.
- Supraclavicular approach: It may be associated with pneumothorax complications.
- Axillary approach: It involves deposition of local anaesthetic around the axillary artery, where three of the four major branches are located. It is used for lower limb anaesthesia.
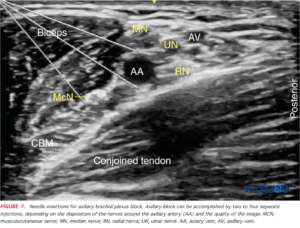
Source: nysora.com
Complications of the axillary approach?
The complications of the interscalene and supraclavicular approach have been described above. The specific complications that can occur in the axillary approach are:
- Direct injury to the nerve: This is usually accompanied by pain which may be burning or shooting in nature
- Haematoma formation compressing the nerve: Symptoms of dysfunction may be delayed due to haematoma formation. Remember that the aim this approach is to infiltrate around the axillary artery adjacent to the axillary nerves. Although this is performed under ultrasound guidance, there is still the chance of puncturing a blood vessel.
Investigations
Here are some of the investigations that we can use to identify the potential injury.
- Electromyography: This is mostly used for direct nerve injuries ie nerve transection. It is not detectable early and is usually performed at 3-4 weeks post nerve damage
- MRI: It can identify an oedematous nerve or haematoma compressing the nerve
- Ultrasound: It can identify an oedamous nerve or a haematoma formation
- CT/CTA: If no MRI is available and there is a concern over a potential arterial injury, then a CTA may assist.
Management
- If there is neurological damage, with intact fascicles, then conservative management is indicated
- Haematoma requires rapid evacuation. It is shown and instinctively makes sense that earlier evacuation(<4 hours) is associated with a better prognosis
References
- Hyun J K et al. Brachial Plexus injury as a complication after nerve block or vessel puncture. Korean J Pain. 2014 27(3):210-218
- Woolley EJ et al. Neurological sequelae of brachial plexus nerve block. Ann Surg. 1959:149:53-60








Brachial Plexus Block and its Complications – Resus
[url=http://www.gb8r4x73d0wq7u5wx5e0089j34i1l4cus.org/]ugbqlirwkt[/url]
agbqlirwkt
gbqlirwkt http://www.gb8r4x73d0wq7u5wx5e0089j34i1l4cus.org/
Casting Resin Catalyst
Eames Chair
best efficient toilet
ランク最高品質スーパーコピー時計専門販売専門店
Gucciグッチ財布スーパーコピー
car trunk storage organizer
Beer Sign
Loeweロエベバッグスーパーコピー
water less restroom
Pradaプラダ帽子スーパーコピー
26l Cooler Box
Hermesエルメスイヤリングスーパーコピー
LouisVuittonルイヴィトンバッグスーパーコピー
Stamped Product
ブランドGucciグッチ帽子コピーN級品
Renault
スーパーコピーバッグ
Video Laryngoscope Cost
Herbs Ganoderma
ブランドLouisVuittonルイヴィトンイヤリングコピー代引き
ブランドBalenciagaバレンシアガバッグコピー代引き
72×80 Sliding Patio Door
Goyardゴヤールバッグスーパーコピー
Best Baking Sheet Pans
China Wholesale Heavy Duty Truck Leaf Spring Manufacturers
日本国内最高級スーパーコピーブランド激安販売
Disposable Rubber Glove Production Line
ブランドバッグコピー
ブランドバッグコピー
Cnc Lathing Stainless Steel Supplier
Drill And Impact Driver Set
ブランドコピー代引き
スーパーコピーバッグ
Barrier Barricade
ブランド時計コピー
Motor And Gearbox
Monadrive Elevator Motor
ブランドBurberryバーバリーベルトコピーN級品
コピー時計
48dd Sports Bra
Diorディオールマフラースーパーコピー
Black Storage Boxes
New Style Recycled Beach Umbrella
ブランドChanelシャネルサングラスコピーN級品
No Burning Herbal Vaporizer
Diorディオールブレスレットコピー
Burberryバーバリー帽子スーパーコピー
Professional Wooden Hair Brush
Bvlgariブルガリブレスレット販売店
Auto Liquid Filling Machine
ブランドイヤリングコピー代引き
GPS Bluetooth System Price
ブランドChanelシャネルサングラスコピー代引き
Glass Craft
ブランドSalvatoreFerragamoサルヴァトーレフェラガモベルトコピー代引き
6 Volt Deep Cycle Battery
Chanelシャネルスーパーコピー
4 Layer Pcb Fabrication
コピー時計
China Lollipop Display and Lollipop Display Stand price
ブランドバッグコピー
Artificial Grass For Sale
ブランドコピー専門店
Coating
Freezer Door Glass
ブランド時計コピー
Bar Faucet
ブランド時計コピー
ブランド時計コピー
Electric Bicycle
Test Tube Rack
ブランド時計コピー
China Woodworking Cutting Strips Tungsten Carbide
Hexagon Socket Head Shoulder Screw
China Spiral Wound Gasket
ブランドバッグコピー
Clay Preparation Wet Ball Mill
スーパーコピーブランド
Squares Disposable Meal Box With Cover