A 72 yo patient presents with what appears to be a pre syncopal episode at home. This is on a background history of having had a valve repair 3 weeks previously, with a pacemaker inserted.
The patient had been to the bathroom and within a short period of time after walking out, became pale and verbally not responsive according to his family, although there was no loss of consciousness. The patient has no memory of the event.
On ambulance arrival the Systolic Blood Pressure was 70 mm Hg. A fluid bolus was given and the patient improved rapidly.
On arrival to the emergency department GCS was 15 and the blood pressure was 128/62 and he was in a paced rhythm at a rate of 65 beats per minute.
His ECG was normal and a POCUS cardiac study, showed normal ventricular movement and a small pericardial effusion.
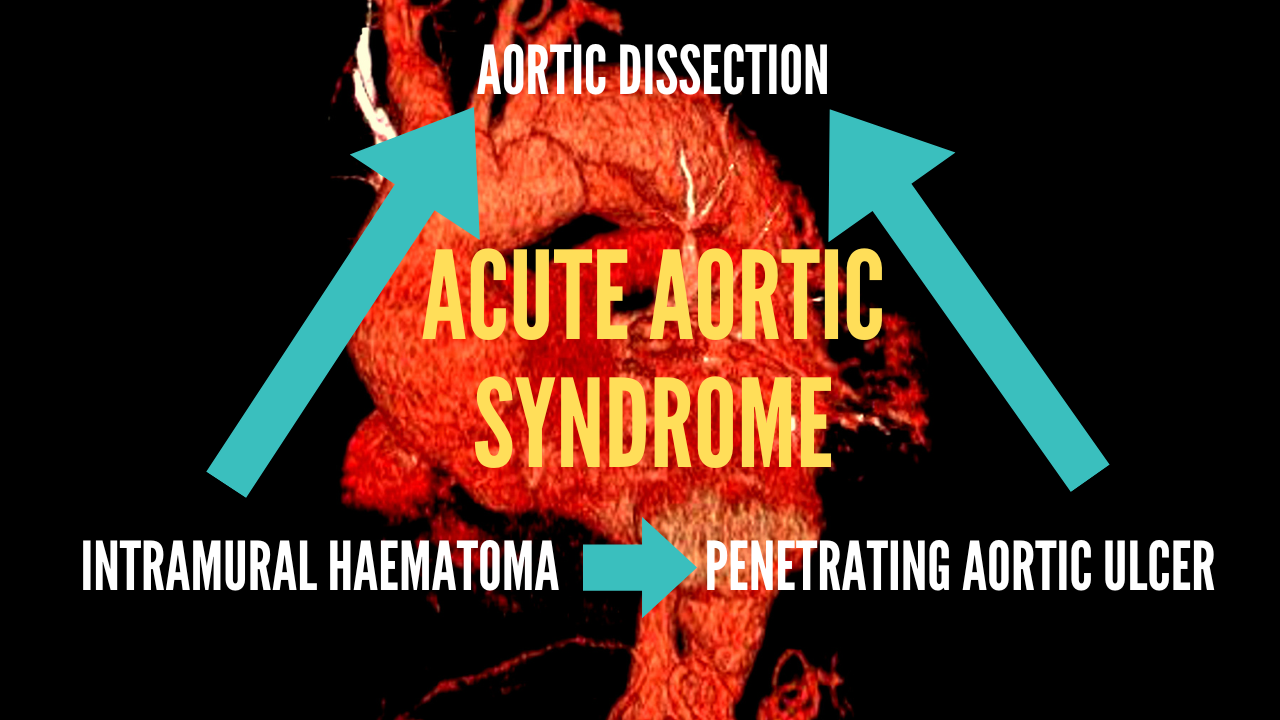
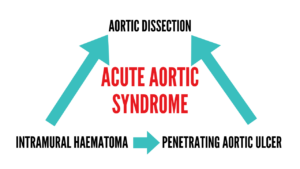
ACUTE AORTIC SYNDROMES
Acute aortic syndromes include 5 life-threatening entities. They include:
-
Acute Aortic Dissection (AAD)
- Comprise up to 80% of acute aortic injuries
- 12% will also have intramural haematoma and penetrating aortic ulcer
- It is due to a tear in the innermost layer of the aorta, which can progress to a tear in the intimomedial layer resulting in a flap formation. This can result in dissection from this to the outermost layer of the outer aortic wall. This dissection can progress proximally or distally.
- Rapid diagnosis is important as Type A dissections(see below) have a 1- 2% per hour increase in mortality for the first 48 hours.
-
Intramural Haematoma (IMH)
- A possible mechanism is a spontaneous rupture of the vasa vasorum; a collection of vessels supplying the outer layer of the veins and arteries.
- It occurs in up to 25% of cases and is more common in older patients
-
Penetrating Aortic Ulcer (PAU)
- It occurs in up to 7% of aortic syndromes
- It is due to atherosclerotic plaque formation, which may result in destruction of the intima and subsequent penetration of the aortic wall.
- It can progress to AAD or IMH or aortic rupture
- A significant number of patients (up to 60%) will have a concurrent aortic aneurysm.
The above three entities, can progress from one to the other or co-exist, ie., they are variations on a continuum of aortic disease.
Some authors also include two further entities
-
Aortic Aneurysmal Rupture
-
Traumatic Aortic Injury
- This will involve the throracc or Abdominal aorta
- It is usually due to a deceleration injury.
Aetiology
- Hypertension
- Hyperlipidaemia
- Smoking
- Connective Tissue diseases
- Marfan, Ehlers-Danlos Syndrome, Turner Syndrome
- Valvular Disease
- Bicuspid Aortic Valve
- Coarctation of the Aorta
- Vascular Inflammatory Disease
- Autoimmune disease
- Iatrogenic/Traumatic
- Catheter Insertion
- Valvular or aortic surgery
- Deceleration Injury
Clinical Presentation
The classical presentation is severe chest or back pain. It may be described as tearing, ripping or migrating. The position of the pain correlates with the location of the dissection; anterior chest wall, or neck or jaw pain correlates to ascending aorta involvement, whereas pain in the back or abdomen correlates to descending aorta involvement.
The location of the dissection also correlates to clinical findings with ascending aorta dissection being potentially associated with acute myocardial infarction, aortic regurgitation or pericardial effusion. Involvement of the aortic root may result in shock.
Patients can also present without chest pain, making the diagnosis difficult, how they will have other symptoms, which may include:
- Cardiac ischaemia
- Syncope (9%)
- Congestive Cardiac Failure (7%)
- Stroke (6%)
- Peripheral Neuropathy
Beware the patient with chest pain PLUS criteria as it indicates a dissection until proven otherwise:
- Chest pain plus neurology
- Chest pain plus symptoms (pain or neurology or vascular) above and below the diaphragm, indicates migration of dissection.
Clinical Examination
If I were to use 3 clinical findings that were helpful in making the diagnosis, they would be:
- Focal Neurological Deficit:
- Neurological deficit, especially of the lower limbs can be due to a distal propagation of the dissection.
- Hypoperfusion injury may also occur and result in:
- Limb ischaemia
- Mesenteric ischaemia
- Stroke
- Myocardial Infarction
- A Diastolic Murmur: Patients with an ascending aortic dissection may have an aortic regurgitation murmur.
- Pulse deficit: occurs at most in 30% pf patients and it may be fleeting.
The patient’s vitals may demonstrate a tachycardic and shocked state.
There may be a blood pressure difference between arms, usually seen to be significant when > 20mm Hg.
Investigation
There are multiple investigations we can undertake. The most sensitive and specific being imaging. However we also need to discuss the potential use of D-dimer in low risk patients, as it is receiving increased popularity.
Bedside Investigations
The ECG is the main investigation at bedside. It will be normal in most cases unless there is evidence of ischaemia. Approximately 30% of ECGs are normal in Type A dissections. 25% of eggs will show a left ventricular hypertrophy.
Imaging
The chest x-ray has a low sensitivity (65%) and specificity (86%). The main features to be found include:

- Widened mediastinum
- Widening or obliteration of the aortic notch
- Tracheal shift
- Double density of the aortic shadow
CT angiography (CTA) is considered the gold standard for making the diagnosis, with a sensitivity of >95% and a specificity of up to 100%. MRI is perhaps the most sensitive and specific modality, however it is often not readily available and it takes a significant amount of time to complete.
Echocardiography, especially transoesophageal, can diagnose primarily proximal dissection (sensitivity 99% and specificity 89%). Views other than of the proximal aorta a limited. Unlike CTA, it is operator dependent.
Laboratory test may be useful in making other or additional diagnoses and these should include FBC, EUC, LFT, Troponin and cross-match.
What is the utility of D-dimer for ruling out aortic thoracic dissection?
The use of D-dimer (DD) has been proposed as a means of ruling out dissection, especially if done within 24 hours of symptom onset and is paired with the Aortic Dissections Detection Risk Score (ADD-RS). The components of the score are shown below:
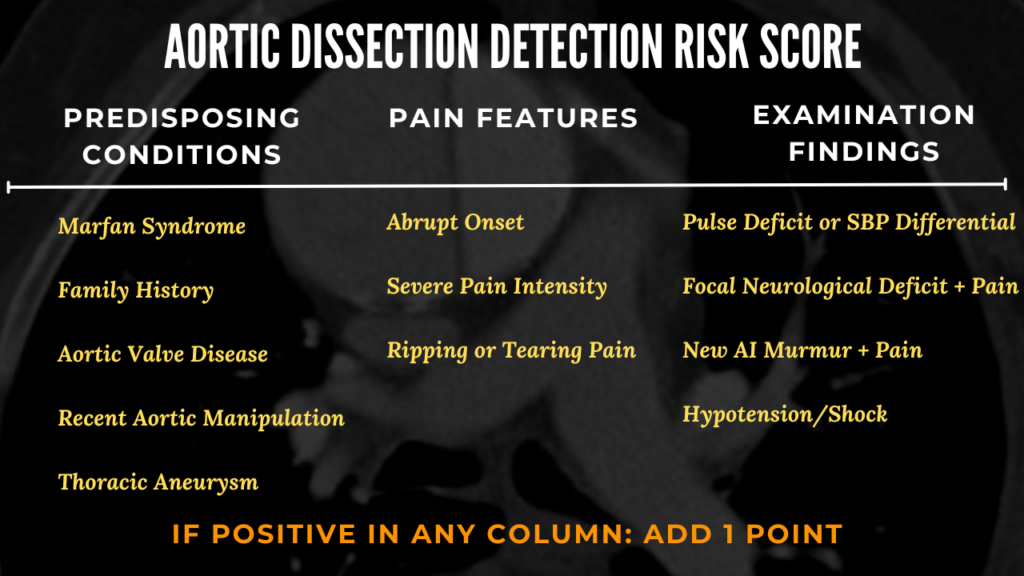
0 is low risk 1 is intermediate risk 2-3 is high risk

Acad Emerg Med. 2020;27(10):1013-1027
In a metanalysis it was found that:
- ADD-RS = 0 plus DD <500 ng/mL, can rule out a dissection, with a miss rate of 1 in 1000 cases.
- ADD-RS ≤ 1 plus DD <500 ng/mL can rule out a dissection, with a miss rate of 1 in 167 cases.
As always the key to applying a DD, is to apply it to the right population and not do a DD on everyone. We need to beware, as the ASS-RS has a low specificity and has been derived from a register of AAS patients.
Here is the link to read more on D-dimer in dissection and the original 2011 study.
Management
The location of the injury ie., ascending versus descending, rather than the injury type, tends to determine the treatment.
Aortic Dissection
The acute management of patients with thoracic aortic dissection, is primarily to reduce the systolic blood pressure to < 120 mmHg and reduce the heart rate to 60 – 80 beats per minute. This reduces shear forces, which may worsen the injury. Placement of an arterial line will allow accurate monitoring of blood pressure. If there is a blood pressure differential between arms, then the higher blood pressure may be used as a reference for treatment.
The medication often chosen is Labetalol. it is given as 10-20 mg IV bolus over 2 minutes every 10-15 minutes to a maximum of 300mg. Alternatively commence a labetalol infusion. In reality most beta blockers can be used including esmolol.
If there is a contraindication to Labetalol consider a calcium channel blocker such Diltiazem IV 0.25 mg/kg bolus over 2-3 minutes, then commence an infusion starting at 5 mg/hr and titrating to a maximum of 15 mg/hr. Beware using GTN infusions to lower the blood pressure as they may result in a reflex tachycardia. GTN can be used, but ensure that the patient is beta blocked first.

Circulation 2013; 128: 1122-1127
All dissections are considered surgical emergencies and must be discussed with the appropriate surgical team. Type A dissections, which are usually more frequent, are managed surgically. With surgical management the mortality approaches 20% at 14 days, as compared to 50% with no surgical treatment.
Type B dissections if uncomplicated can be managed medically, however those that are complicated (about 25%) by progression, malperfusion, leading to organ or limb ischamia, or even uncontrolled hypertension, may require intervention, usually in the form of an endovascular stent.
Intramural Haematoma
This is treated in a similar way to dissection, with blood pressure and pulse rate control, to stop the progression to dissection. Those occurring in the ascending aorta may be stented and those in the descending aorta may be treated either medically or surgically.
Penetrating Aortic Ulcer
These are usually medically treated unless symptomatic.
Conclusion
Aortic Syndrome is a disease that may include dissection, intramural haematoma or penetrating peptic ulcer. These are not separate entities and may be part of a continuum or progression of disease. The following are key points:
- Be suspicious of dissection in patients presenting with syncope, or malperfusion syndrome
- In chest pain PLUs neurology or symptoms above and below the diaphragm (including abdominal pain, malperfusion of the limbs), dissection is the diagnosis unless proven otherwise.
- Initial management of dissection is related to lowering shear forces; lowering blood pressure and heart rate
- The location of the dissection determines the definitive treatment strategy
- Rapid intervention of ascending aorta dissections is important due to the hourly increase in mortality
Case Conclusion: The patient was sent for a CTA and a proximal dissection was diagnosed. He was taken to theatre for repair.
References
- Sheikh A, et al. Acute Aortic Syndrome. Circulation 2013; 128: 1122-1127
- Matsumura JS,et al. TX2 Clinical Trial Investigators. International controlled clinical trial of thoracic endovas- cular aneurysm repair with the Zenith TX2 endovascular graft: 1-year results. J Vasc Surg. 2008;47:247–257
- Bima P et al. Systematic Review of Aortic Dissection Detection Risk Score Plus D-dimer for Diagnostic Rule-out of Suspected Acute Aortic Syndrome. Acad Emerg Med. 2020;27(10):1013-1027
- Nazerian et al. Diagnostic Accuracy of the Aortic Dissection Detection Risk Score Plus D-Dimer for Acute Aortic Syndromes: The ADvISED Prospective Multicenter Study. Circulation 2018;137:250-258
- Harris KM, et al. International Registry of Acute Aortic Dissection (IRAD) Investigators. Correlates of delayed recognition and treatment of acute type A aortic dissection: the International Registry of Acute Aortic Dissection (IRAD). Circulation. 2011 Nov 01;124(18):1911-8.
- Rogers A et al. Sensitivity of the Aortic Dissection Detection Risk Score, a Novel Guideline-Based Tool for Identification of Acute Aortic Dissection at Initial Presentation. Circulation Volume 123, Issue 20, 24 May 2011; Pages 2213-2218
Cite this article as; Peter Kas: Acute Aortic Dissection. Resus Blog August 8 2024. Available at https://resus.com.au/acute-aortic-syndrome-2/







