A 58 yo patient presents with abdominal pain. No cause is found for the pain, however the patient was admitted, for overnight observation.
An initial ECG is shown below. Is there anything concerning in this ECG?
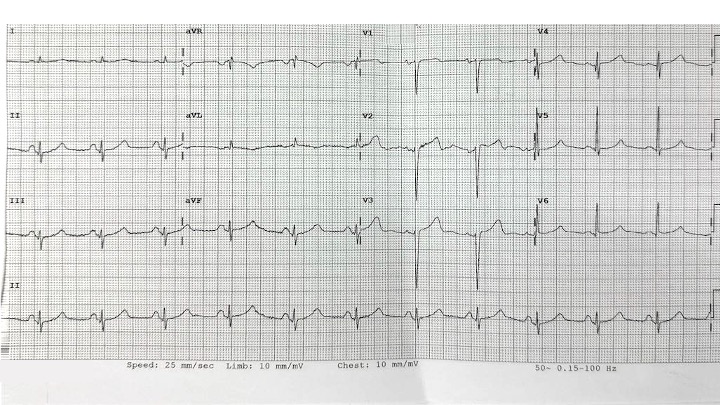
My initial thoughts are that if I was concerned about cardiac ischaemia, there would be a few things that were concerning about this ECG, in terms of potential ischaemia:
- There is an Upright T wave in V1: Usually the T wave in V1 is inverted. Usually to be concerned about ischaemia, I would expect that the T wave in V1>V6
- There is T wave inversion in aVL
At Cardiac Bootcamp I teach the 11 things to look for in potential ‘sneaky ischaemia’.
They include the following:
- Reciprocal ECG changes
- Hyperacute T4 WAVES- “t wave TOWERS over R wave”
- T wave inversion in aVL
- ST Segment is Straight of Convex: Think Ischaemia
- Terminal QRS distortion- sometimes called the QRT sign
- New upright T wave in V1 >V6
- U wave with opposite polarity to T wave
- Serial ECGs catch sneaky ischaemia- especially Wellen’s
- STE can occur in non-contiguous leads- South African Flag Sign
An ECG taken 4 hours later is shown below. Are there any concerns now?
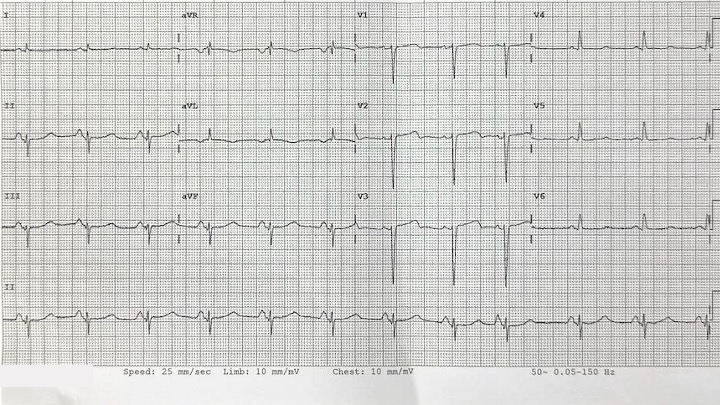
The changes are very similar, although now there is more of a biphasic waveform in V2.
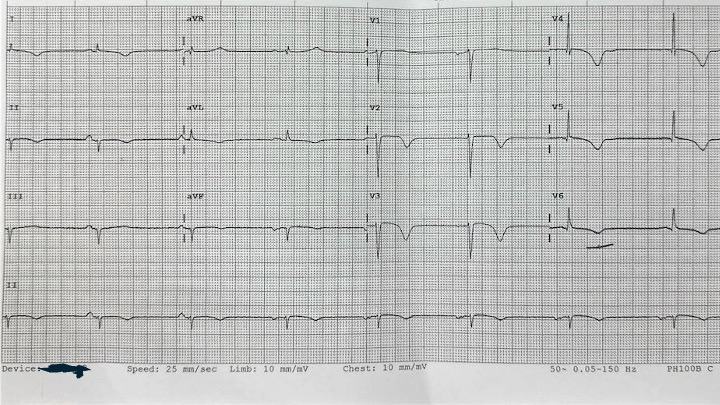
An ECG taken 8 hours later is shown below. There is no doubt about the ischaemic pattern now. The patient had a very significant troponin leak.
Learning Points from this Case:
- Beware abdominal pain, especially in older patients, as it may be cardiac ischaemia in disguise.
- Use the ‘Sneaky Ischaemia’ hints







