
He has no relevant past medical history.
Hi ECG is shown below:
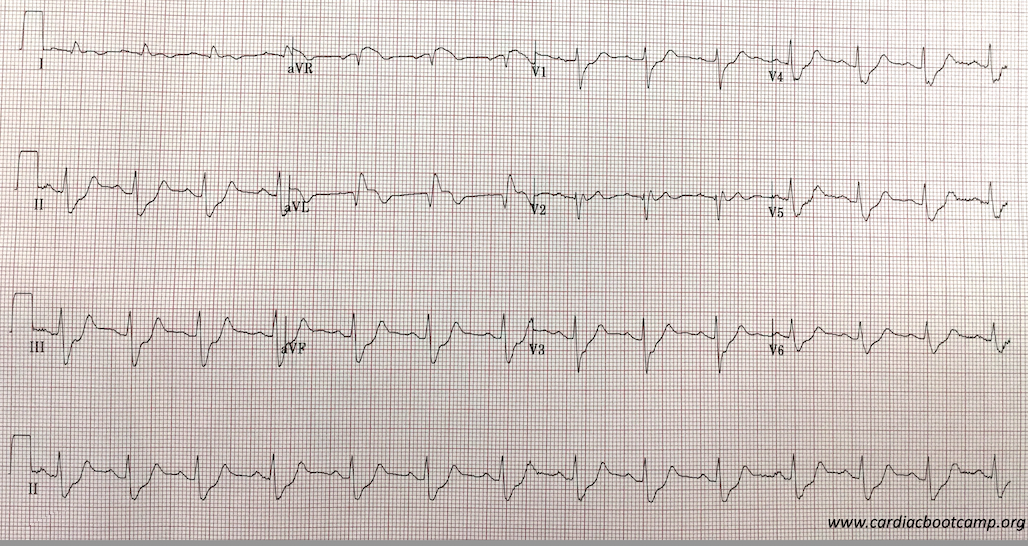
You diagnose a probable LAD occlusion and that the patient is in cardiogenic shock. Your hospital doesn’t have a Cath lab and so you decide to thrombolyse. However, you also need to sort out the cardiac failure and the blood pressure.
GTN is not an option to dilate due to the cariogenic shock. You decide on CPAP for the breathing but need to support the blood pressure. What do you use?
- Adrenaline
- Noradrenaline
- Dopamine
- Isoprenaline
- Dobutamine
- Milrinone
- Vassopressin
Some Important Comments in the LiteratureIs one Pressor better than the other? Perhaps another question to ask is if one pressor, although efficacious in the short term lead to worst outcome? By this I mean, something that may work well right now, but lead to worst outcomes a week or two down the track when the patient is out of the emergency department.
The Cochrane Review first published findings in 2016 of Vasopressors in hypotensive shock and said”
“We found no evidence of substantial differences in total mortality between several vasopressors. Dopamine increases the risk of arrhythmia compared with norepinephrine and might increase mortality. Otherwise, evidence of any other differences between any of the six vasopressors examined is insufficient.”
Cochrane Database of Systematic reviewsTarvasmaki et al, in an observational study in Critical Care (2016) 20:208 found that patients on Adrenaline had a worst survival and an increased 90 day mortality compared to other vasopressors. However the study didn’t prove causality and a prospective trial is needed.
In a comparison of Dopamine and Noradrenaline in the treatment of shock, De Baker et al (NEJM 2010;362(9):779) found that although not significant, there was a trend towards a higher death rate when Dopamine was used. There were certainly a significant number of adverse events such as arrhythmias, when Dopamine was used. In a sub-group analysis in this same study they found that in cariogenic shock, Noradrenaline was superior to dopamine in terms of reduction in mortality.
This was the case of the 65 yo male in CARDIOGENIC SHOCK.
The optimal treatment for this patient would have been to start NorAdrenaline and then add Dobutamine, especially as there was no previous history of heart disease. Milrinone may be a substitute in patients with known poor ejection fraction ie., known significant heart failure.
The key is to start with Noradrenaline.
A quick review of the Medications available
α1 = vascular(arterial) smooth muscle
β1 = Heart: Increases rate and force of contraction
β2 = Bronchial Smooth muscle dilatation
INOPRESSORS: Adrenaline and NorAdrenaline
Adrenaline (αβββ)
Non-selective adrenergic agonist: acts on α and β receptors. At low doses, acts on β2 receptors causing vasodilation. At higher doses its effect on α1 and β1, resulting in positive inotropy and vasoconstriction( of peripheral vasculature and pulmonary arterial and venous circulation).
It is both a chronotrope and an inotrope
It’s use is mostly in anaphylaxis and cardiac arrest as other drug combinations have been found to be better for both septic and cariogenic shock.
NorAdrenaline(αααβ)
It acts on vascular α1 adrenergic receptors, causing vasoconstriction and thus increasing systolic and diastolic blood pressures. It has chronotropic and inotropic effects by acting on on cardiac α1 receptors.
It can cause tachycardia and increase myocardial oxygen demand. It may also have a direct toxic effect on cardiac cells. It is the first line management of septic shock and may be used with other medications.
INODILATORS: Dobutamine and Milrinone
Dobutamine (αββ)
Dobutamine, a synthetic catecholamine, acts on β1 receptors increasing cardiac contractility. It also has α1 and β1 effects on peripheral vasculature resulting in vasodilatation at lower doses, thus increasing cardiac output. At doses above 5mcg/kg/min it can result in vasoconstriction.
It is usually used with an inopressor in cariogenic shock.
A meta-analysis, showed Dobutamine to be associated with higher in-hospital mortality and readmission rates for heart failure exacerbation when compared to nesiritide therapy. Higher doses of dobutamine is not preferred in patients with recent myocardial ischemia, as it can increase myocardial oxygen demand and induce tachycardia.
Milrinone
It is a Phosphodiesterase Type 3 inhibitor(PDE3) used inotropic agent in patients with cardiogenic shock. It inhibits PDE3, which results in more calcium ions entering the myocardial cell, increasing cardiac contractility. It also acts on peripheral and pulmonary vasculature leading to vasodilatation as well as inotropic effect. It does not act on the beta adrenergic pathway.
Another feature of the mechanism of action of milrinone is that the same intracellular processes is activated in smooth muscle cells of the peripheral and pulmonary vasculature, leading to a net vasodilatory effect in addition to its positive inotropic effect.
In a sub-group analysis of the OPTIME-CHF trial, it was found to increase mortality in patients w
ith heart failure of ischaemic origin.
Conclusion:
Think about the medications you are using in cardiogenic shock.
Start with Noradrenaline and then add to that. In most cases it will be Dobutamine.







