A22yomale presents to the emergency department with a history of lethargy, fatigue and palpitations. He has no chest pain or SOB.
There is no past medical history.
The patient believes he feels like this, as he had a big gym workout today.
An ECG is done because of the history of palpitations. What is your interpretation?
There is no past medical history.
The patient believes he feels like this, as he had a big gym workout today.
An ECG is done because of the history of palpitations. What is your interpretation?
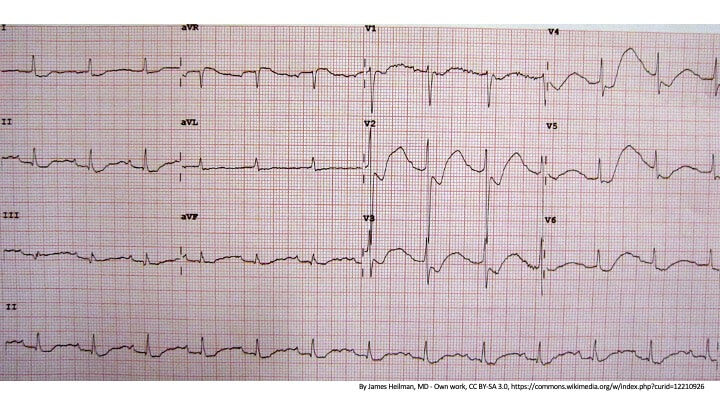
Sinus Rhythm at rate of 98bpm
Normal QRS width
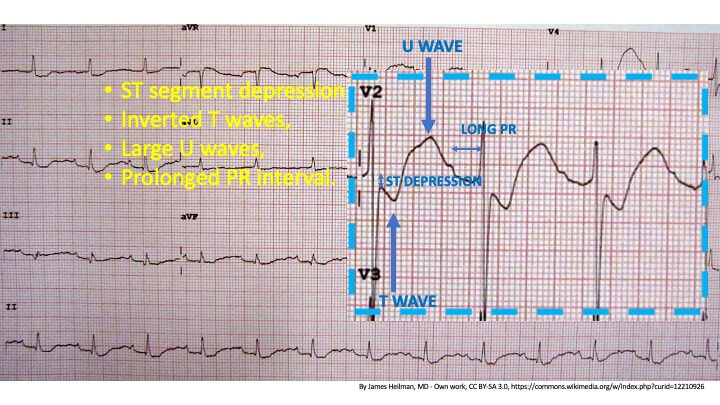
Widespread ST depression I, II, aVL aVF V1-V6 with abnormal ST segments due to?
Intervals: PR is prolonged, Is that a long QT?
Normal QRS width
Widespread ST depression I, II, aVL aVF V1-V6 with abnormal ST segments due to?
Intervals: PR is prolonged, Is that a long QT?
- What is the diagnosis?
- What is the potential cause in this patient?
- If this patient went into Torsades de Pointes, following cardioversion with electricity, would you treat with:
- Amiodarone or
- Magnesium?
- What are the causes generally?
- What conditions is this ECG pattern mistaken for?
….answers are below.
This is the classic ECG of hypokalaemia. It has the 4 classic changes:
- ST segment Depression
- Inverted T waves
- Large U waves
- Prolonged PR Interval
Beware here as there is no prolonged QT, but a long QU due to the prominent U waves.
See the ECG Below for these changes. The patient’s potassium was 1.1 mmol/L
Diagnosis
This patient has Hypokalaemic Periodic Paralysis. It is characterised by muscle weakness of the shoulders and hips associated with hypokalaemia.
Proximal Weakness is usually greater than distal weakness. The respiratory muscles are usually spared, although they may not be.
The conditions presents with first attacks in childhood and adolescence. A first attack in someone older than 25 years is almost never this condition, unless it is associated with thyrotoxic periodic paralysis.
It has an autosomal dominant inheritance.
Attacks are precipitated by:
Proximal Weakness is usually greater than distal weakness. The respiratory muscles are usually spared, although they may not be.
The conditions presents with first attacks in childhood and adolescence. A first attack in someone older than 25 years is almost never this condition, unless it is associated with thyrotoxic periodic paralysis.
It has an autosomal dominant inheritance.
Attacks are precipitated by:
- High carbohydrate meal
- Rest following Exercise
- High Na Content Foods
- Sudden Change in Temperature
Clinical Diagnosis is made by:
- Episodes of Paralysis
- Low K during attacks but normal between
- Triggers
- Familial History
Patients tend to develop a progressive myopathy over time.
If this patient went into Torsades de Pointes, following
cardioversion with electricity, what would you treat with?
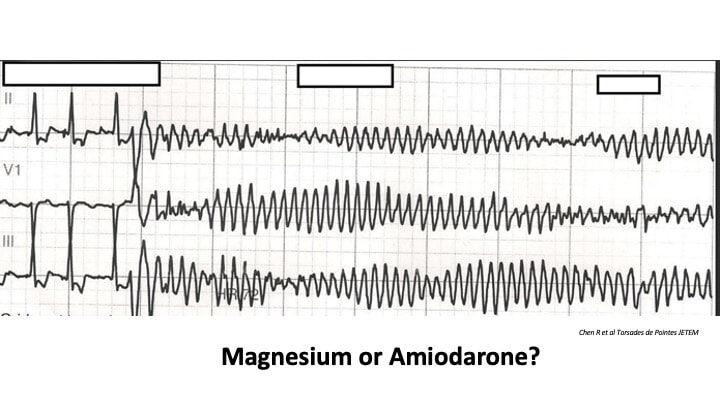
Obviously we would need to treat the hypokalaemia. However rapid correction of hypokalaemia can result in ventricular arrhythmias and asystole.
Usually patients with hypokalaemia also have hypomagnesaemia. Magnesium is modulator of K+ ion transport.
Therefore GIVE MAGNESIUM.
Usually patients with hypokalaemia also have hypomagnesaemia. Magnesium is modulator of K+ ion transport.
Therefore GIVE MAGNESIUM.
What are the Causes and What ischaemic condition is it
sometimes mistaken for?
Go to the Hypokalaemia section of the cardiac Course and see more cases, causes and what it is mistaken for.







