
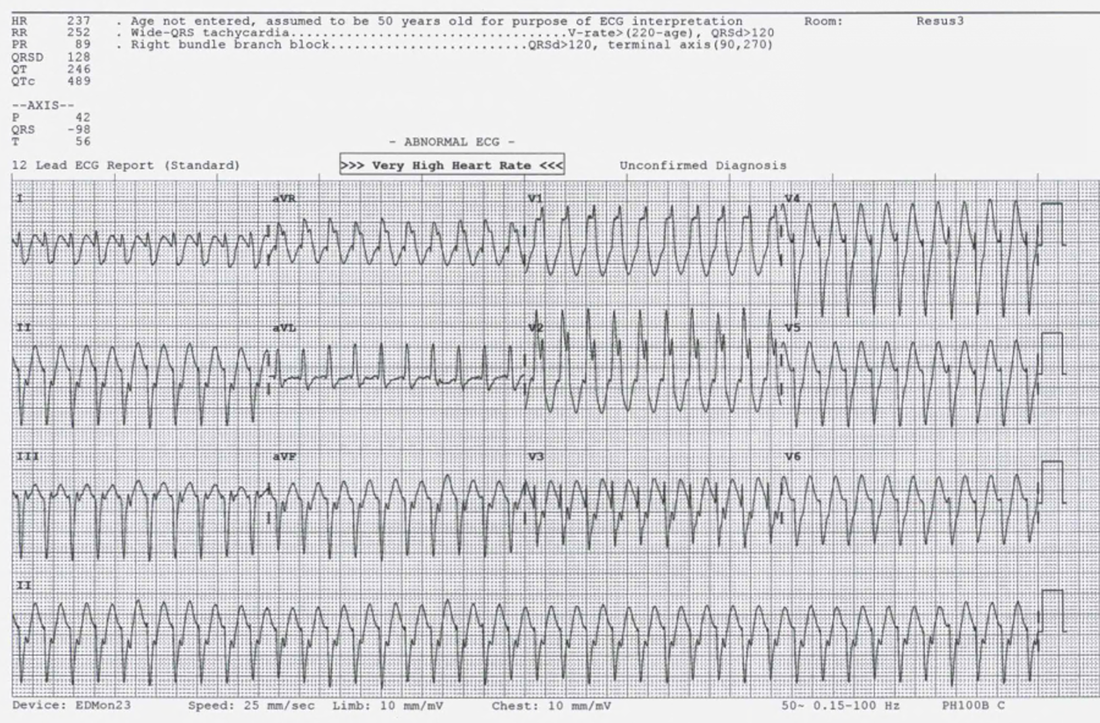
He is afebrile, with a respiratory rate of 14 a heart rate of 237bpm and a blood pressure of 119/67.
An ECG is done and is shown below.
What does the ECG show and what is your diagnosis?
Is it Ventricular Tachycardia?
ANSWER
This is a wide ‘ish’ complex tachycardia at a rate of 237bpm. There is a RBBB morphology.
The axis is extreme.
If we use the 120 CRAM formula to see if it VT:
Faster than 120bpm (but not too fast)- It is faster than 120.
Wider than 120ms- It is borderline.
Concordance: No
Initial R wave in aVR: No
AV Dissociation: No
Morphology: RBBB pattern however there is an rsR pattern not indicative of VT
R/S > 1
I would consider this more likely to be Supraventricular Tachycardia (SVT) with a RBBB, even with the axis as it is.
How would you manage this haemodynamically stable patient?
(b) Cardioversion
(c) Sotalol IV
(d) Amiodarone
ANSWER
This can be a difficult question to answer. For those who prefer cardioversion in every patient with a WCT, that’s a very appropriate approach..
However, is there any harm in giving Adenosine? There are 3 things to consider:
- If this was VT, the adenosine would have no effect (unless an idiopathic VT, but we will leave that for the moment.
- If it is SVT with RBBB, it would hopefully revert the arrhythmia
- Given that the rate is very fast, could there be an accessory pathway?
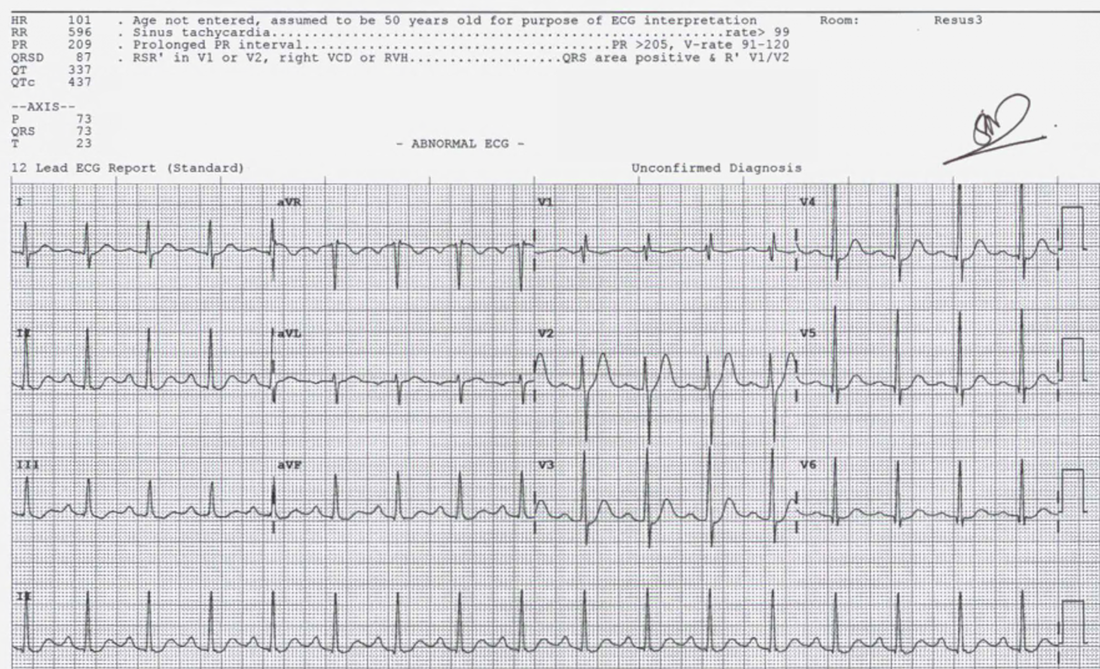
The patient was given Adenosine and reverted as shown below. Was this an Idiopathic Ventricular Tachycardia. How do you differentiate it from Ventricular tachycardia or from an SVT with aberrancy?
What is Idiopathic Ventricular Tachycardia?
Idiopathic Ventricular Tachycardia (VT), occurs in structurally normal hearts and comprises about 10% of VT cases. This is a more benign form of VT, with patients rarely suffering from sudden cardiac death. Definitive treatment includes medications or ablation.
Patients presenting to the emergency department with this arrhythmia, can be cardioverted and some will respond to AV nodal blockers such as Adenosine or Calcium Channel Blockers or Beta Blockers. However, even if the arrhythmia reverts with these, the patient should still be discussed with cardiology, especially if they fit the particular ECG patterns discussed below. Idiopathic VT can be mistaken for a supra ventricular tachycardia(SVT) with aberrancy and it will respond in some cases to AV nodal blockers, just like an SVT with aberrancy, so beware. However there are some distinct differences in morphology and axis, that allow us to identify it.
Classifications can be confusing. For simplicity we can classify them as:
- Outflow tract VT (right or Left)
- Idiopathic Left Ventricular tachycardia or fascicular tachycardia
Below is a schematic on identification of each type.
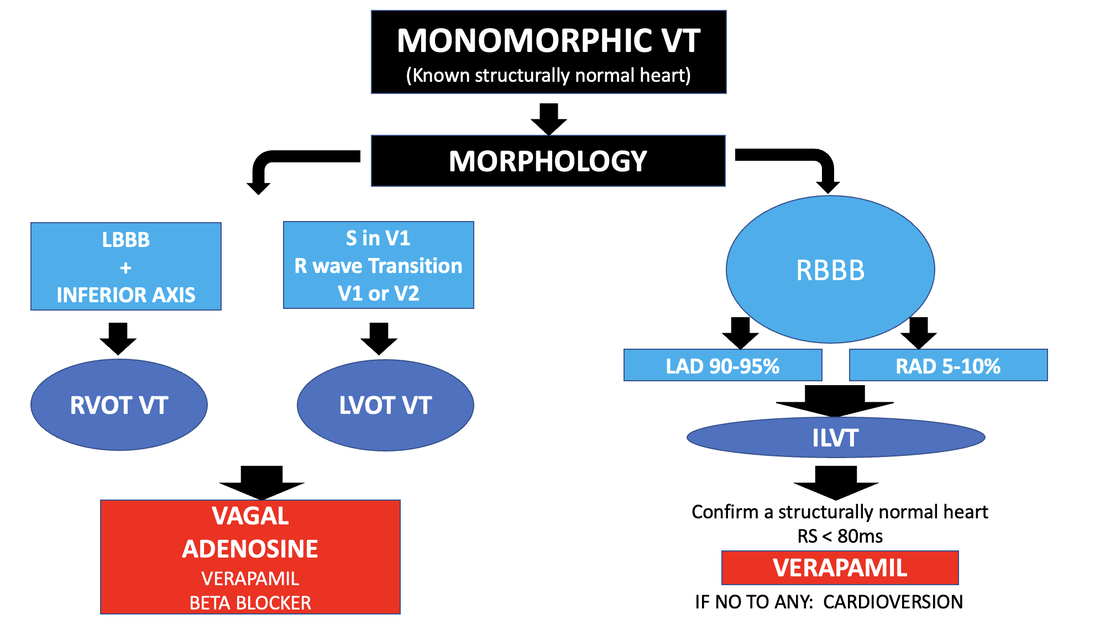








Simple and sweet explanation