
Introduction
When we assume that every wide complex tachycardia is Ventricular Tachycardia(VT) our sensitivity for picking up VT is 100%. In the emergency department setting, this is a must! We use electricity on all of these patients because it is safe and effective. We can try adenosine, in case it’s a supra ventricular tachycardia(SVT) but only if it’s a regular rhythm.
Our specificity in this scenario lags, however in our favour, is that fact that 80% of WCT is VT. If we wanted to determine if an ECG is showing VT, we have a range of rules at our disposal, including Brugada and Vereckei, that give a respectable specificity, but it’s still in the mid 80%.
A new validated rule
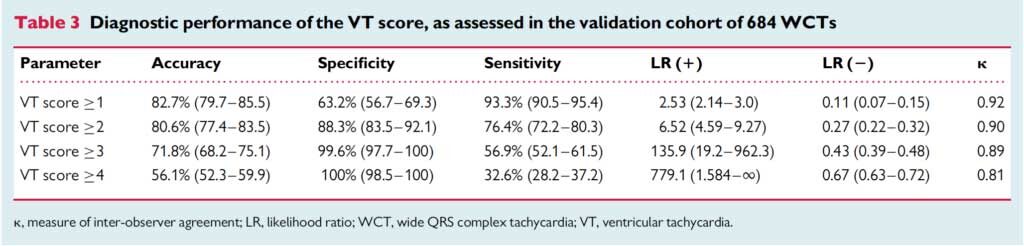
The VT Score, uses 7 criteria, some of which we already use, to diagnose VT. A specificity of 100% is reached when 4 or more criteria are satisfied(1).
When we assume that every wide complex tachycardia is Ventricular Tachycardia(VT) our sensitivity for picking up VT is 100%. In the emergency department setting, this is a must! We use electricity on all of these patients because it is safe and effective. We can try adenosine, in case it’s a supra ventricular tachycardia(SVT) but only if it’s a regular rhythm.
Our specificity in this scenario lags, however in our favour, is that fact that 80% of WCT is VT. If we wanted to determine if an ECG is showing VT, we have a range of rules at our disposal, including Brugada and Vereckei, that give a respectable specificity, but it’s still in the mid 80%.
A new validated rule
The VT Score, uses 7 criteria, some of which we already use, to diagnose VT. A specificity of 100% is reached when 4 or more criteria are satisfied(1).
The Seven Criteria are as follows:
NOTE: Before we start I would add that the rate should be greater than 120 beats per minute for us to start considering VT.
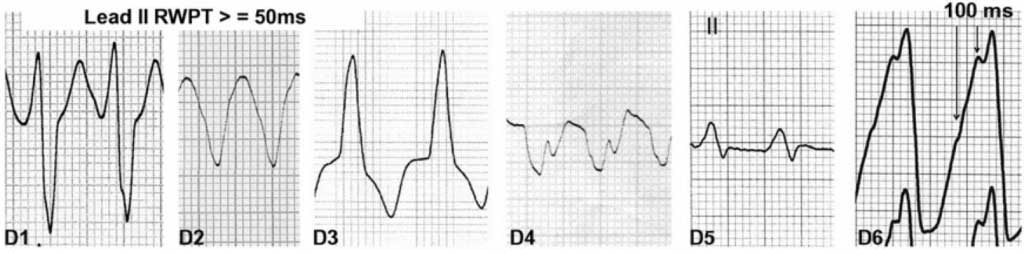
1. Dominant Initial R wave in V1. This can be notched(the original rabbit’s ear) provided the notch is on the descending limb.
NOTE: Before we start I would add that the rate should be greater than 120 beats per minute for us to start considering VT.
1. Dominant Initial R wave in V1. This can be notched(the original rabbit’s ear) provided the notch is on the descending limb.
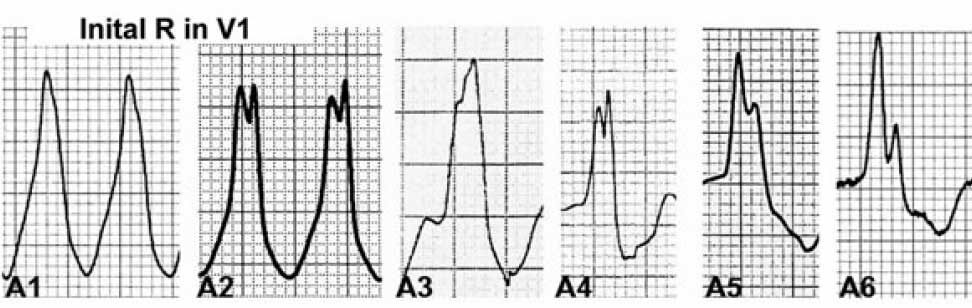
2. Initial r > 40 ms in V1 or V2: assess in predominantly negative QRS complexes. Look for a ‘fat’ initial r in rS in V1. It can also include variations such as: RS with high ‘r’ amplitude, rS with notched r

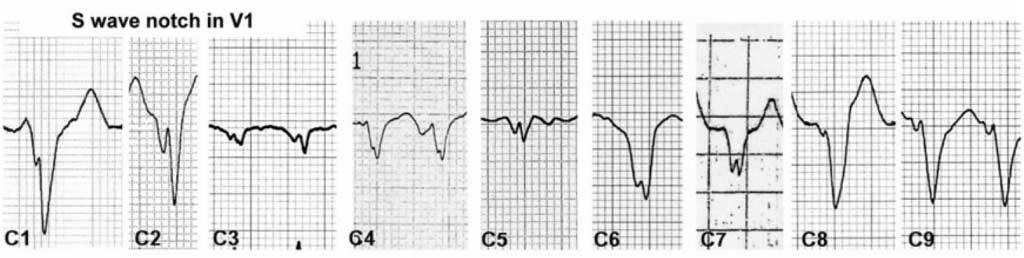
3 Notched S in V1. The notch can be at the beginning, in the middle or near the nadir of the S wave.(This has been known as Josephson’s Sign)
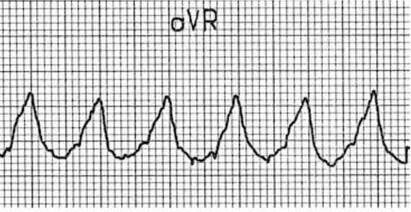
4. Initial R wave in aVR. The QRS in aVR must start with a large R wave. it can be notched. (This comes from the Vereckei(2) criteria).
5. Lead II R wave Peak time(RWPT) > or equal to 50ms. This is the time from the beginning of QRS to first change in direction.
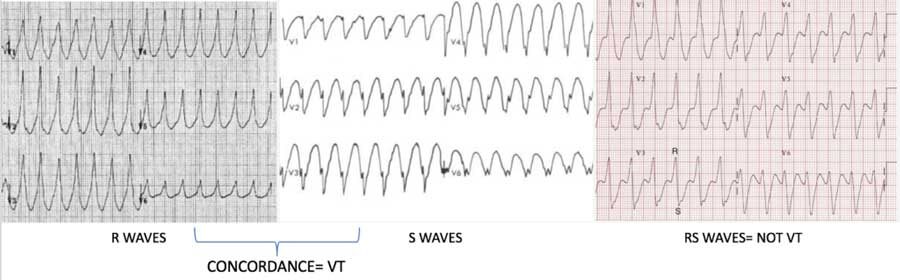
6. Lack of RS in V1-V6.(Brugada Criterion(3)). This is similar to saying that there is concordance.
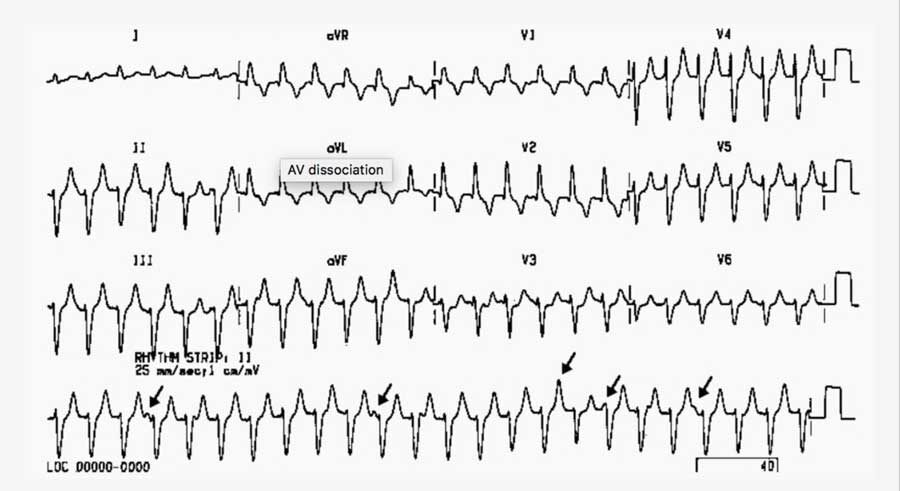
7. Atrioventricular Dissociation. This is indicated where a fast ventricular activity iOS not related to atrial depolarisation.
Source: LITFL
LETS MAKE IT EASIER TO REMEMBER:
- Rate must be > 120bpm to be VT
- Concordance in V1-V6
- AV Dissociation
- Josephson’s Sign in V1 -V2
- Look at V1 for a FAT INITIAL R wave (r>40ms) this could be the rabbits ear
- Look at aVR for a FAT Wave to begin with
- Look at lead II RWPT > 50ms- again a big R wave.
References
- Jastrzebski M et al. The ventricular tachycardia score: a novel approach to electrocardiographic diagnosis of ventricular tachycardia. Europace. 2016 Apr;18(4):578-84
- Vereckei A et al. Application of a new algorithm in the differential diagnosis of wide QRS complex tachycardia. Eur Heart J 2007.28:589-600
- Brugada P. et al. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation 1991:83:1649-1659







