This blog is based on a case study in the literature.
A 60 yo male with a recent previous history of angina (with a cardiac stent), has intermittent left sided chest pain. His past medical history is Hypertension and Diabetes. He is haemodynamically stable with a heart rate of 93bpm and Blood Pressure of 122/80 and a respiratory rate of 18.
His ECG shows Q waves in leads III and aVF and his troponin is normal.
4 hours later he crashes, becomes diaphoretic and tachypnoeic, with a heart rate of 136 bpm and a BP of 70mmHg.
An ECG is done and shown below. Based on this, the patient is taken to the cath lab.
What does it show? What is the diagnosis?
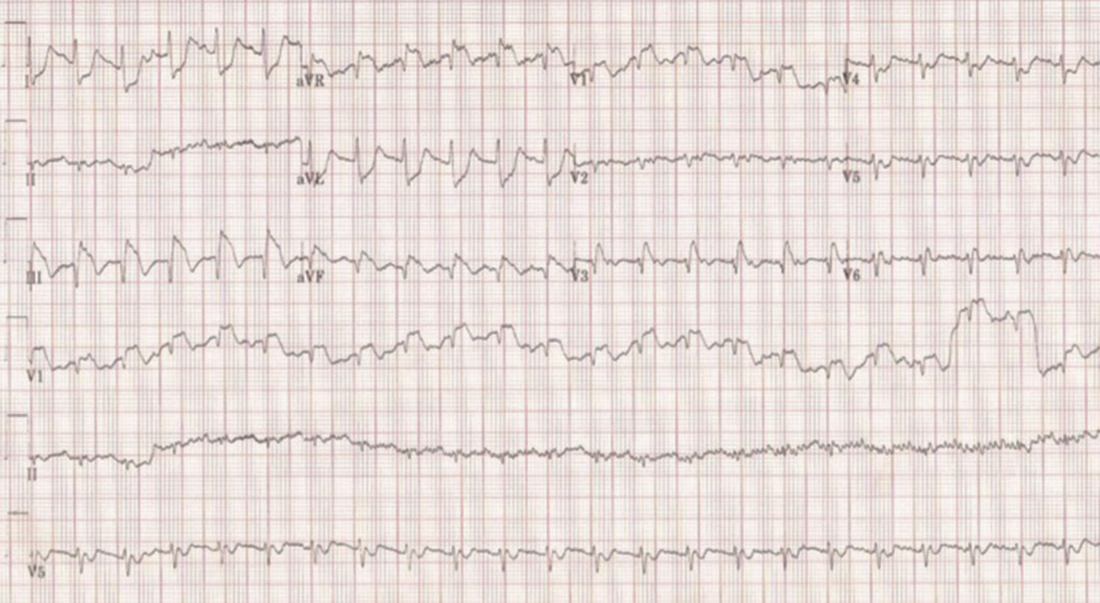
- Sinus tachycardia
- ST elevation in III, aVF and aVR and V1 with reciprocal changes in precordial leads and lateral leads. The ST elevation and reciprocal changes are consistent with a STEMI
Can you see anything else?
…. There is an S1Q3T3
A CTPA was done that revealed a large saddle pulmonary embolism.
Let’s look at PE mimicking an acute infarction.
Clinical Presentation of PE
Match the following percentages with the following symptoms:
79%, 57%, 47%, 26%
- Pleuritic chest pain
- Tachycardia
- Tachypnoea
- New dyspnoea at rest or exertion
- Pleuritic chest pain. 47%
- Tachycardia. 26%
- Tachypnoea. 57%
- New dyspnoea at rest or exertion. 79%
What are some of the ECG Findings in PE?
Findings on ECG, for the most, are non-specific for diagnosing pulmonary embolism.
Some of the more typical findings include:
- Sinus Tachycardia
- S1Q3T3
- S1Q3
- Right Axis
- Bundle Branch Block (complete or incomplete)
- T wave inversions in the right precordial leads (right heart strain).
Other ECG abnormalities
In a study by Sreeram et al, it was found that > 3 of the following increased probability of PE:
- RBBB (complete or incomplete) + STE and positive T wave in V1
- Right axis deviation
- S waves >1.5mm in I and aVL
- Shift of transition zone in precordial leads to V5
- Q waves in III and aVF (but not II)
- T wave inversion in III, aVF, V1-4
- Low voltage QRS in limb leads of <5mm
It’s hard to remember everything
You can’t remember everything, so look these up next time a patient presents. The ECG must be looked at with the patient’s presenting complaint and past history.
I remember to look for 5 things:
- Unexplained Sinus Tachycardia
- S1Q3T3 or S1Q3
- RBBB (complete or incomplete) + right axis deviation
- T wave inversion in III and V1-4
- S wave in I (+ aVL)
Topics on Pulmonary embolism in the members section include:
- The ECGs of Pulmonary Embolism
- ECG findings that predict your patient is about to crash
- What are the symptoms and clinical signs of pulmonary embolism?
- Scoring systems
- Investigations such as the ABG and D-dimer
- PE in Pregnancy
- What about sub-segmental PE’s?
- Who needs thrombolysis?
- The most important studies in management of PE
REFERENCES
-
- Villablanca P A et al. Case report and systematic review of pulmonary embolism mimicking ST-elevation myocardial infarction. Vascular 2019, Vol 27(I) 90-97.
- Falterman TJ, et al. Pulmonary embolism with ST segment elevation in leads V1 to V4: case report and review of the literature regarding electrocardiographic changes in acute pulmonary embolism. J Emerg Med 2001; 21: 255–261.
- Sreeram N, et al. Value of the 12-lead electrocardiogram at hospital admission in the diagnosis of pulmonary embolism. Am J Cardiol 1994; 73: 298–303.
- Villablanca P A et al. Case report and systematic review of pulmonary embolism mimicking ST-elevation myocardial infarction. Vascular 2019, Vol 27(I) 90-97.







