
The Case
A 40 yo is brought to the emergency department with the following vitals:
- GCS 4
- SBP 70mmHg
- HR 140
- RR 50
- T 39C
There are no signs of injury. Heart sounds are dual and no extra sounds. There are reduced breath sounds and crepitations in the left base. The abdomen is soft and the patient appears to have peripheral cyanosis.
The patient has a known history of IVDU and has been found in a chair, not rousable.
She has fluids and inotropes and antibiotics and she has the ECG shown.
What are your differential diagnoses for this patient? What is the most likely diagnosis?
The computer says acute AMI. Could it be?
Let’s look at the ECG
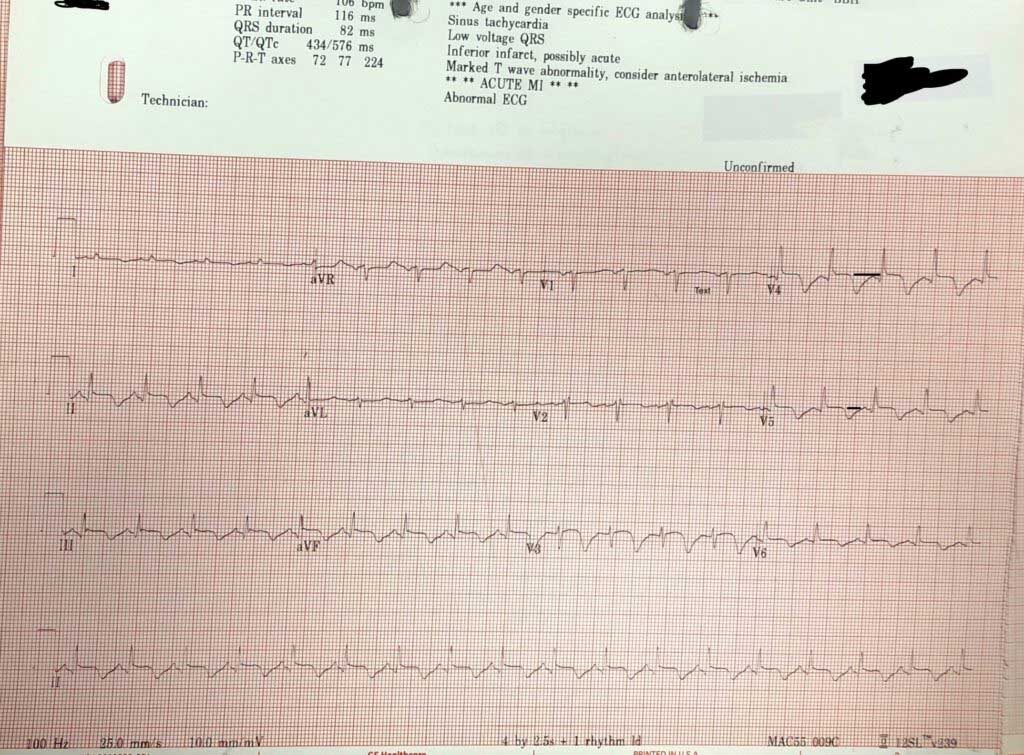
Rate 106
Is it sinus?– P waves are upright in II and inverted in aVR; Yes
Is there a P for every QRS? Yes
QRS:
Is it tall/small?: It’s about right, there is no hypertrophy.
Is it wide/narrow? It’s narrow
Is it of abnormal morphology ie., delta wave? No
Is it clumped?(just incase we miss a Mobitz- but it’s not slow enough) No
ST-T
Remember the baseline is the T-P line
If we look we see that there is some ST elevation in some areas of the ECG of about 1mm, although this is difficult to gauge as the T wave goes straight into the p wave.
The most visible abnormality is the inverted T waves.
What causes inverted T waves?As this is an adult patient we can overlook the T wave inversion of childhood. Other prominent causes are:
- Acute Myocardial Infarction
- Ventricular Hypertrophy( not present on this ECG)
- Pulmonary Embolism
- Raised Intracranial Pressure( I would usually expect them to be deeper)
PR and QT Intervals
The PR is normal and the QT is very prolonged.
PACING Spikes: None.
Putting it all together, what would seem the most probable diagnosis?Before we look at the most likely diagnoses. One differential to entertain is an overdose, however there are no signs of classic QRS widening of Na channel blockade, or a terminal R wave in aVR.
It might be an AMI, there is no evidence of hypertrophy, the patient is not behaving like they have a PE, but they may have raised intracranial pressure given the decreased conscious state. The decreased conscious state may be simply due to low blood pressure.
The patient is also febrile. Why? Remember this patient has a history of IVDU, so infective endocarditis is a consideration. The patient may also have meningitis. The fever may also be secondary to stroke as we know that about 50% of stroke develop a fever, which in itself is a marker of severity and marker of mortality.
Let’s narrow it down to 2 causes, AMI and raised intracranial pressure. Raised intracranial pressure ECG’s have deep T wave inversion and a prolonged QT. I’m thinking this is an intracranial event, especially if the fever is due to this.
Echo showed a myocardium, not contraction properly, with clean valves, so it may be AMI. However the CT gave the diagnosis with large subarachnoid haemorrhage.
This is a neurocardiogenic phenomenon when the heart is affected by deranged autonomic supply coming from a stroke. A fascinating case mixed with electrolyte abnormalities etc. I hope you enjoyed it.








Most likely ,the patient is in carcinogenic shock following Antero-Lateral MI and now sepsis or could the patient have viral infection to the heart valves ???