Syncope is not uncommon, occurring in up to 25% of children. Most causes are benign, however we need to be aware of the of 3 major groups as these can be very serious diagnoses:
- Those with a cardiac cause
- Those with a neurological cause
- Very young children, as syncope shouldn’t occur in this group.
Making the diagnosis in children can be stressful, so I like to use a simple algorithmic approach to work through the possible diagnoses. This is primarily so I don’t not miss the more important causes. (For a review of adult syncope and the ECG’s of syncope click here) There are syncope rules in existence, however these apply to adult patients.
Definition of Syncope
Syncope in children and adults is a symptom, not a condition. It is up to us to determine the cause. The definition of syncope involves three components:
- Loss of consciousness
- Loss of postural tone
- Recovery and return to baseline
This third part of the definition is important. Simple neurocardiogenic syncope will have a return to baseline usually within about 30 seconds, perhaps a little longer in the elderly. However if there is altered consciousness for more than about 5 minutes, then seizure or other neurological cause needs to be considered.
Below is a great example of syncope. A child at a spelling bee, loses consciousness, collapses to the ground and then very rapidly makes a recovery to baseline and continues spelling the word given.




Cardiac Causes of Syncope
These are not common, occurring in up to 6% of children, however they are potentially the most serious causes. They include the following groups:
- Those with Cardiac structural abnormalities
- Valvular defects
- Patent foramens
- Previous cardiac surgery
- Outflow Obstruction: left or right
- Arrhythmias
- Bradycardias: These can include complete heart block and are usually due to:
- Rheumatic Fever
- Myocarditis
- Endocarditis
- Ventricular Tachycardia: This can be due to congenital defects, electrolyte disturbances, drugs or myocarditis.
- Bradycardias: These can include complete heart block and are usually due to:
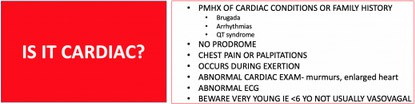
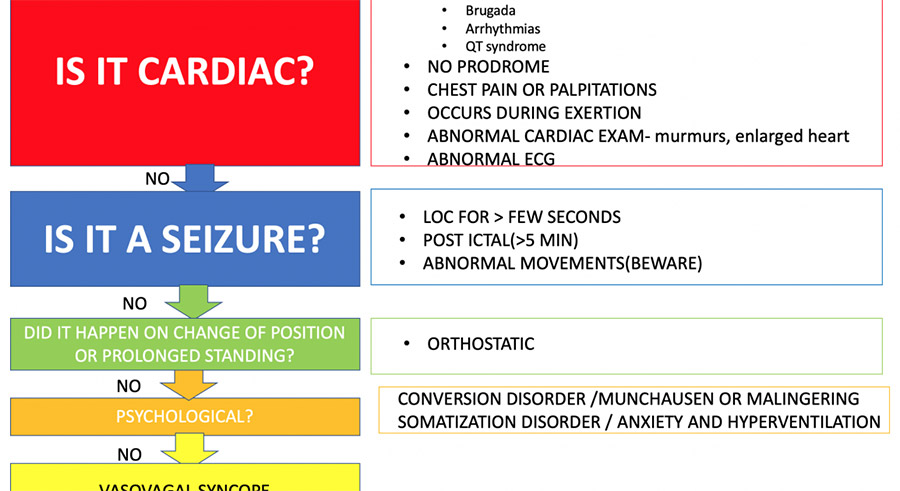
Red Flags for Cardiac Syncope
- Syncope occurs DURING exertion(rather than after exertion)
- There may have been chest pain or palpitations
- The patient has a murmur
- There may be congenital heart disease
- There may be a familial History of
- long QT Syndrome (read the case on the 9 yo with syncope)
- Sudden death
- Cardiomyopathy
Neurological Causes of Syncope
Neurological causes of syncope need to be considered, especially if there is a post-ictal component. Patients that have a simple syncopal episode secondary to vasovagal causes, usually recover very quickly. Patients that are confused for more than 5 minutes need to be considered as having had a seizure.
Patients that have a non-neurological cause of syncope usually collapse and then have abnormal movements, that are usually anoxia-related and may be mistaken for seizures. Those patients that have true seizures, usually seize and then drop. There are some exceptions to this, which include atonic seizures, which usually have no prodrome, however this is a good approach to the patient where seizures are described.
Vascular events need to also be considered. These may include vertebrobasilar insufficiency, or subclavian steal syndrome. A thorough history of activities related to the event must also be sought, given that on occasions activities involving purposeful valsalva and even vascular obstruction, with ‘choking games’ can result in collapse.
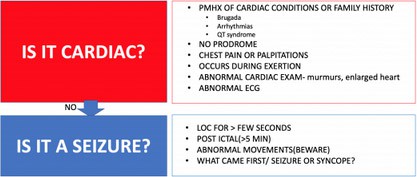
Red Flags for Neurological Causes
- Neurological symptoms
- Post ictal state
- Injuries to Lip/Tongue
- Urinary Incontinence
Check for Orthostatic Hypotension
Psychological Causes of Syncope
Up to 25% of syncope is due to psychological causes, which can include anxiety and depression, conversion and somatisation disorders.
Patients with conversion disorder, can have multiple events with normal vitals and examination. Those with somatisation disorder will usually have multiple other complaints.
Neurocardiogenic Syncope
This is what we generally refer to as vasovagal syncope. It is usually secondary to an abnormal vasodilatation, resulting in a drop in blood pressure, which leads to dizziness, light-headedness and collapse.
Other Conditions to Think About
There are many other conditions we can discuss, however one common one is breath holding spells. These occur in up to about 5% of toddlers and are benign, but can be very upsetting when first seen.
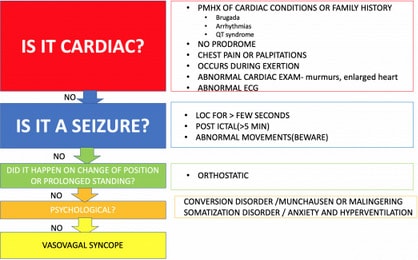
An Approach
History
A good history will give the diagnosis in most cases. Seek the red flags of cardiac or neurological syncope. Ask about family history. Is there a psychiatric history, or is there a suspected psychiatric cause for the syncope?
Examination
As always vitals are important. Think about heart rate; too slow a rate may indicate a heart block.
Are there any murmurs? Is there any orthostatic hypotension?
Investigations
There aren’t too many investigations that assist. Certainly the ECG is the most important investigation. It has a low yield, however when positive gives the diagnosis. Laboratory investigations might include a full blood count and bHCG.
Work through the algorithm above. It isn’t exhaustive and we should always use good clinical judgement.
Peter Kas