CASE
A 72 yo woman presents to your emergency department following an episode of syncope. There was a brief 2-3 seconds of dizziness followed by a loss of consciousness. The patient did not complain of chest pain or palpitations, nor headache, nor abdominal pain and there was no weakness, or loss of function. There was no loss of bladder or bowel control and collateral history did not reveal any mention of seizure activity. The patient recovered totally in just over 2 minutes.
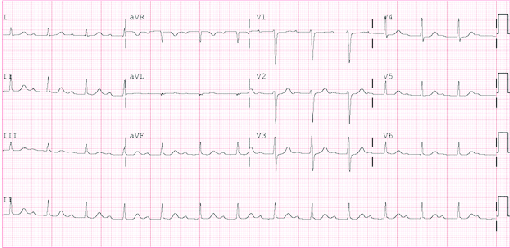
Past Medical History includes hypertension. Examination is normal. ECG shows a first degree heart block
Does this patient have an increased risk of arrhythmia? What do we do with this patient?
A new study may shed some light.
I’ve written about syncope in adults and children about syncope rules and the ECG’s of syncope before (watch the videos below).
We have seen in most of the literature, that age is an independent predictor of risk as is a cardiac cause of syncope, with cardiac causes identifying a much higher risk or mortality than other causes.
With respect to the elderly, approximately 6% with undifferentiated causes of syncope presenting to the emergency department, will have a serious adverse event, including death, within 30 days of that presentation(1).
What does this new study show?
Nishijima et al(2) looked at ECG findings that are predictive of adverse events in the elderly. An abnormal ECG had a 77.9% sensitivity and a 46.6% specificity for predicting a serious arrhythmia within 30 days. They found that the following ECG findings were predictors of serious cardiac arrhythmias:
- Non-sinus rhythm (OR 2.8)
- Multiple Premature Ventricular Conductions (OR 2.4)
- Short PR (OR 2.7)
- First degree AV Conduction Block (OR1.9)
- Complete Left Bundle Branch Block (OR 2.4)
- Q/ST/T segment abnormalities consistent with acute or chronic ischaemia (OR 1.8)
Snapshot of the Study
- Prospective Observational
- Patients older than 60 years of age
- n=3613
- Primary Outcome: Serious cardiac arrhythmias identified within 30 days of index ED evaluation
- Interesting result: 104 patients(3%) had a serious arrhythmia within 30 days of their ED visit, not identified at the initial ED visit
- Limitations
- Potential sampling bias, as convenience sample used
- Only about half of patients consented to the study
- ECG’s not read by ED physicians, may have affected the results
What do I take away from this study?
As we have seen before, anything that is an abnormal ECG, can be a significant predictor of pathology, especially in the elderly. What is abnormal? …..Anything that is not normal sinus rhythm.
This study identifies some abnormalities that we may not have associated with increased risk, such as first degree heart block.
What we don’t know from this study, is whether admitting these patients makes any difference.
References
- Sun BC, et al. Predictors of 30-day serious events in older patients with syncope. Ann Emerg Med. 2009;54:769-778
- Nishijima DK. et al. ECG Predictors of Cardiac Arrhythmias in Older Adults with Syncope. Ann Emerg Med. 2018;71:452-461








ECG predictors of Cardiac Arrhythmias in Elderly with Syncope – Resus
akoimsggkk
koimsggkk http://www.g6l876qln9gkkjmz5103u183oa6o2l60s.org/
[url=http://www.g6l876qln9gkkjmz5103u183oa6o2l60s.org/]ukoimsggkk[/url]
6000 watt pure sine wave inverter
Lamb Fillet Cooking Time
Alternator
評判の良いコピー機複合機のメーカーはどこですかランド
Coloring Book Printing
LouisVuittonルイヴィトンサングラススーパーコピー
Gucciグッチバッグスーパーコピー
Led Display Screen For Shop
Hermesエルメスバッグスーパーコピー
Large Soft Play Equipment
Diorディオールバッグスーパーコピー
Progressive Plastic Semi Finished Lens
LouisVuittonルイヴィトンバッグスーパーコピー
portable toilet service
Chanelシャネルバッグスーパーコピー
Cnc Copper Busbar Milling
Hermesエルメス靴スーパーコピー
water efficient toilet bowl
Gucciグッチ帽子スーパーコピー
A3 Printing Machine
Led Pendant Light
ブランドGoyardゴヤール財布コピーN級品
Hermesエルメスベルト販売店
Standing Lamp
Fpc Switch Circuit
ブランドコピー代引き
Emergency Light Self
高級リアルドール
Beautiful Cutting Boards
スーパーコピーブランド
Technical Ceramics
ブランドバッグコピー
スーパーコピーブランド
All In One Interactive Flat Panel
Ganoderma Lucidum Essence
Diorディオール帽子販売店
Pet Pvc Clamshell
SaintLaurentサンローランコピー激安
ブランド財布コピー
C Shape Commercial Artificial Lawn
Pradaプラダバッグスーパーコピー
Automated Shelving System
Cellulose Pill Capsules
ブランドBreitlingブライトリング時計コピー代引き
12709880013 Repair Kit
スーパーコピーブランド
Card Customization Supplier
Tiffanyティファニーブランドコピー代引き
SaintLaurentサンローランバッグコピー
Fipronil 80% WDG
5 Stage Hydraulic Cylinder
スーパーコピーバッグ
ブランドBottegaVenetaボッテガヴェネタ靴コピー代引き
4g Sim Card Gps Tracker With Diagnostic Function Micro Bike Motorcycle Gps Tracking Device Gps Tracker
ブランドコピー専門店
304 Steel Sheet Metal
スーパーコピーバッグ
Humidifier Portable
Berenstein Catheter
スーパーコピーブランド
ブランドコピー代引き
Car Park Sensor System
ブランド時計コピー
Portable Slit Lamp Microscope
ブランドコピー専門店
Carbide Solutions
Zinc Oxide Powder For Medical Ointment
A106b
Paracord Camera Shoulder Neck Strap
ブランドコピー代引き
Best Sunglasses
Flake Knife Plastic Crusher
ブランドコピー専門店