We often start with a case and talk about a single topic. This case is a little different. It is a real-time case. What would you do with this patient every step along the way? In real life, things are not always clear-cut. Here’s the story of a man that walked into a hole and then came into the emergency department.
CASE
A 75 yo male presents with a small abrasion to the head, after what appears to be a mechanical fall. The patient describes in detail the fact that he lost his footing and fell. There was no syncope, no loss of consciousness, just a mechanical fall.
The patient has a previous history of Bipolar Disorder, Congestive cardiac Failure and a Non-ST Elevation Myocardial Infarction 2 years previously(NSTEMI).
His medications include Lithium, allopurinol frusemide and spironolactone.
His Vitals are: HR 120 , RR 14, BP 122/82, T 37.2, SpO2 93%
His examination is relatively unremarkable, Hs dual, chest clear, slight tremor otherwise Near is normal.
His ECG is shown below. What is your reading?
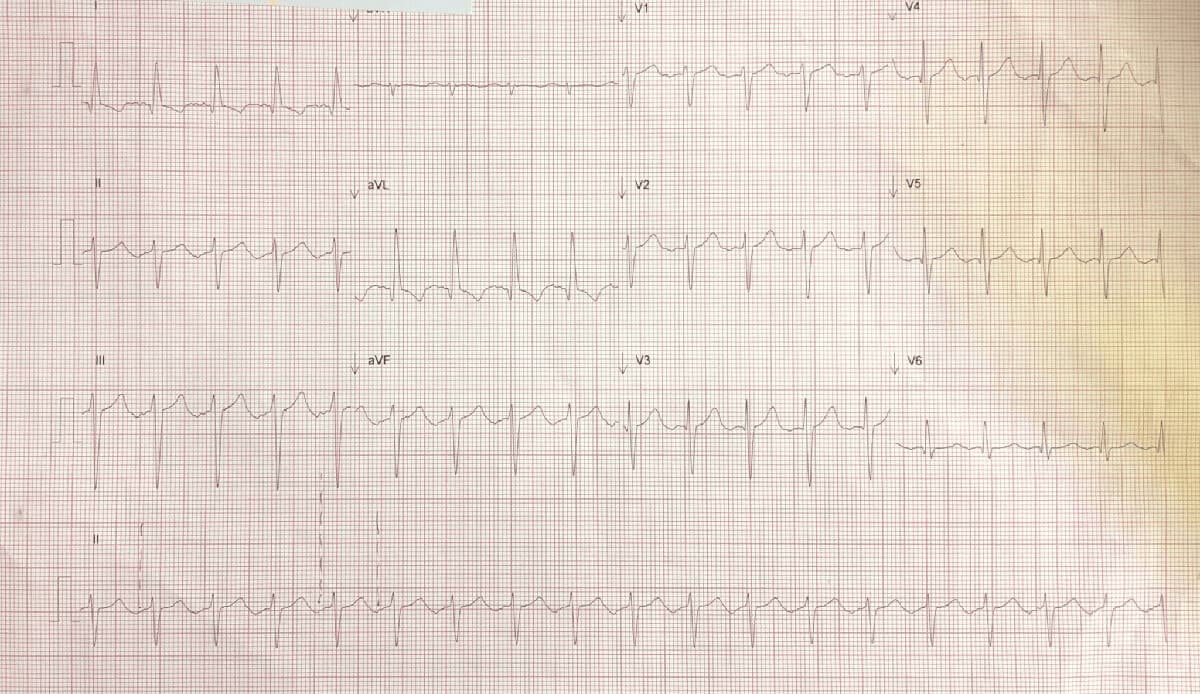
My reading of this is sinus rhythm(I can see p waves) at a rate of 114bpm. There is T wave inversion in I and aVL and the QTc is 531ms, a concern. What is the significance of the ECG changes in someone without chest pain?
Can Lithium cause the ECG changes?
Lithium toxicity can cause supra ventricular and ventricular arrhythmias. Bradycardia as well as supraventricular tachycardia and ventricular tachycardia and fibrillation have been described. The waves may be flattened sometimes inverted and there is a prolonged QTcorrected. (1,2).
The patient isn’t Lithium toxic. Perhaps some T wave changes may be caused by Lithium, however the T wave inversion is in I and aVL, a defined territory and not widespread.
Do we have an old ECG to compare with?
Yes two years previously.
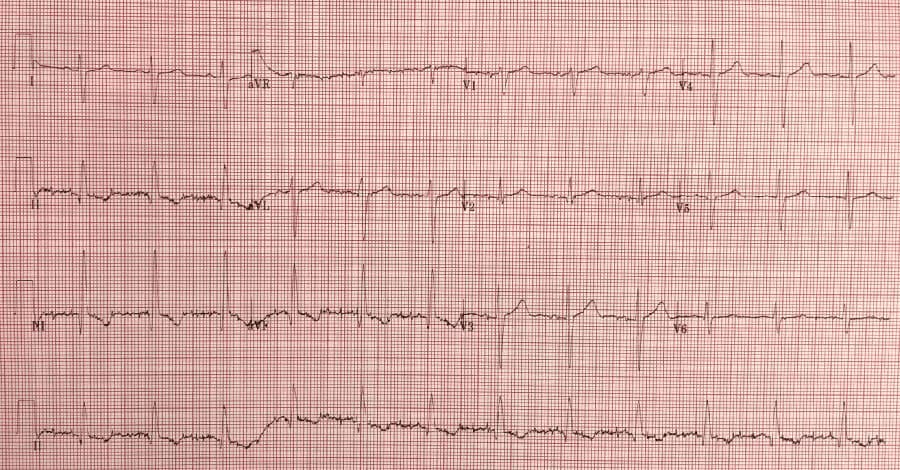
In this ECG, the patient has had inferior T wave inversions but no changes in I or aVL
This looks like an old inferior infarction.
The patient’s blood tests results return:
Na 140
K 4.1
Cl 103
Bic 31
U 4.9
Creat 129 (64-108)
eGFR 46 (>60)
Li 0.96(0.5-0.8)
Someone had added a Troponin, that came back as 0.056(<0.04)
Can Lithium Cause Renal Changes?
Lithium can cause renal changes, however these tend to be with chronic use, rather than acute toxicity. The most common is nephrogenic diabetes insipidus(NDI) and chronic tubulointerstitial nephropathy, the second causing renal insufficiency, but only a small chance of progression to end stage renal failure. Chronic lithium ingestion can lead to NDI, which results in polyuria and polydipsia.
The above results show a chronic effect of lithium on the kidney function
Can Lithium Cause Troponin Changes?
The troponin is raised.
- Could this be as a result of the renal impairment?
- Could it be ischaemic? ie., real?
- Could it be due to the Lithium?
Lithium is not associated with increases in cardiac biomarkers.
Is the raised troponin related to a the raised Creatinine? It may be. The way to rule this out is to perform a serial Troponin and see if it rises further. A serial Troponin came back at 0.071- this was real, primarily because it had rapidly changed over a short period of time, it confirmed that it wasn’t renal. Another possibility, would be to take a CKMB as this is not usually raised by renal impairment.
So Is this all ischaemic? My belief was that together with the ECG findings this may have been real. The patient’s cardiologist stated that a recent cardiac angiogram was normal. So why the T wave inversions? Could this be a Type 2 cause of Troponin rise, secondary to the ongoing tachycardia?
Do we give a patient on Lithium, Aspirin?
This patient has not had chest pain, however there is a Troponin rise, some may argue for aspirin. There is concern over giving NSAID’s in patient’s with any renal impairment taking Lithium as they can affect the clearance of Lithium, resulting in raised Lithium levels. Aspirin however is an exception. It doesn’t appear to affect the lithium levels.
Does this patient need it? A single dose until we decide what is going on, will not hurt the patient. I would start it.
References
- White B, Larry J, Kantharia BK. Protracted presyncope and profound bradycardia due to lithium toxicity. Int J Cardiol 2008; 125:e48.
- Mayra Gonçalves Menegueti et al. Severe arrhythmia after lithium intoxication in a patient with bipolar disorder admitted to the intensive care unit. Indian J Crit Care Med. 2012 Apr-Jun; 16(2): 109–111.








If this patient is already on Aspirin (NSTEMI PCI;2 years ago) is there any value in giving him another Aspirin?