BLUNT CARDIAC INJURY
When should we investigate the patient with suspected blunt cardiac injury (BCI) and how do we work them up?
The evidence in this area is mostly made up of retrospective studies and case studies. The main areas of uncertainty involve:
- How significant both non-displaced and displaced sternal fractures are
- The significance of a post sternal fracture haematoma
- The use of ECG and Troponin as screening tests
- The use of transoesophageal echocardiography as part of the investigations for making the diagnosis in all patients.
Here are some clinical scenarios to consider. What would you do?
A 60 year old patient presents following a motor vehicle accident, with associated thoracic impact.
- There are no thoracic injuries found but the patient is having frequent PVCs on the monitor. Would you be concerned for BCI in this patient?
- What if the same patient had no PVCs, a normal ECG but a slightly raised(25% above normal) High sensitivity troponin? Would you be concerned for BCI in this patient?
- What if the patient had multiple rib fractures and a small haemothorax. Would your threshold to workup for BCI increase significantly?
- If the patient only had a sternal fracture +/- displacement, how concerned would you be for a BCI?
BCI is thought of as cardiac injury resulting from thoracic trauma. There is no clear definition. An understanding of when to work up suspected BCI is important as the mortality is as high as 30% (1).
The Americal Association of Surgery and Trauma (AAST) (1) define five grades of injury ranging from Grade I which is minor ECG abnormalities such as PVC’s or ST-T Changes, or a persistent tachycardia, to Garde VI, which is blunt avulsion of the heart. This grading system does not really help us with an approach to the suspected diagnosis.
MECHANISMS THAT CAN LEAD TO BCI (3, 4)
- Direct chest injuries
- Acceleration-deceleration injuries that result in torsion of attachment points of the heart
- Sternal fractures leading to cardiac compression (read below for the literature on this)
- Indirect blast injuries
The resultant injuries to the heart can be:
- Ventricular or atrial wall injury, including laceration and rupture
- Papillary muscle rupture
- Ischaemia from coronary artery damage
More significant injuries that can lead to early mortality include; rupture of the right or left ventricles, and right atrial rupture.
CLINICAL FINDINGS THAT MAY INDICATE BCI
BCI tends to be associated with more complex thoracic injuries including:
- Haemothorax
- Pneumothorax
- Multiple rib fractures
- Flail chest
- Aortic injuries
- Pulmonary contusions
Patients can clinically present with a number of abnormalities, however they can also initially be asymptomatic. Presentations include:
- Arrhythmias
- Unexplained tachycardias
- PVCs or PACs
- New murmurs
- Unexplained hypotension
- Acute heart failure
- Acute myocardial ischaemia
- Wall hypokinesis
- Abnormal ECG findings including:
- AVN blocks
- RBBB
- ST Segment changes
ARE PATIENTS WITH STERNAL FRACTURES AT HIGH RISK OF BCI?
We have always approached sternal fractures, especially if displaced, as high risk for BCI, due to the potential for compression of the heart against the vertebral column. However most of the literature on sternal fractures and BCI is retrospective and much of it is contradictory.
De Waele et al (5) in a retrospective study found that the incidence of BCI in isolated sternal fractures to be as high as 32%. Approximately one third of those patients had displaced fractures. Although not as high a rate, Athanassiadi K et al (6) found that there is a 4% incidence of BCI in isolated sternal fractures and this was diagnosed on abnormal ECG.
In contrast, Fokin et al(7) in a retrospective study of 380 patients of which 68 had isolated sternal fractures, found that none of these patients had a BCI.
Heidelberg et al (8) in a retrospective review of 235 patients in a single center, found no increase in BCI with sternal displacement, as compared to non-displaced fractures. They also found, as did Rashid et al (9) that retrosternal haematomas were not associated with BCI.
In the geriatric population(10) there may be an association between existing cardiac disease and sternal fractures.
HOW SHOULD WE APPROACH ISOLATED STERNAL FRACTURES?
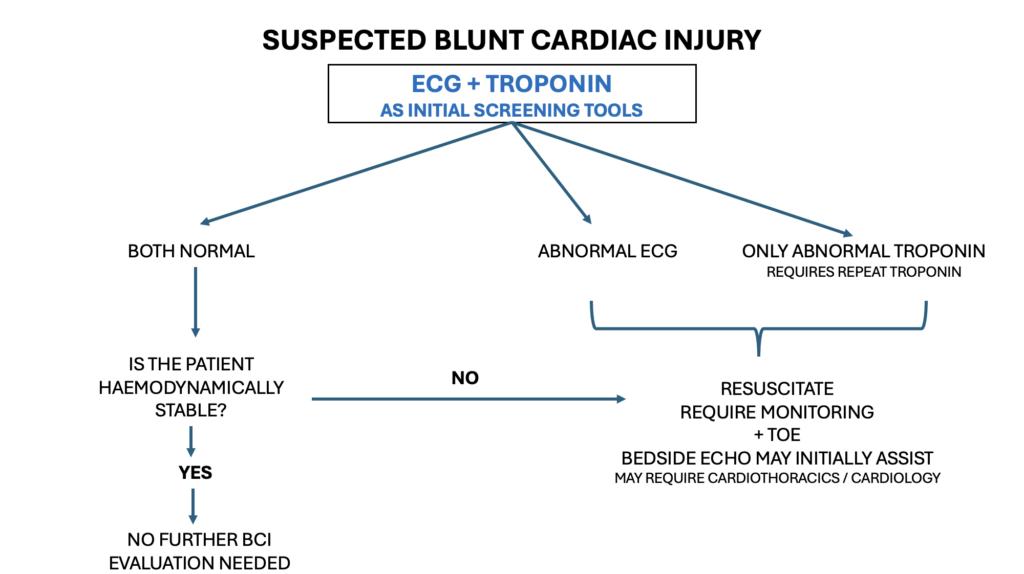
This is where it becomes a little harder. There is a move away from working up isolated sternal fractures, however the evidence (some of which is presented below) is not robust. Due to this reason, my approach is to perform an ECG and high sensitivity troponin on patients with suspected BCI due to mechanism and clinical presentation. This are simple and inexpensive tests that can give us a lot of information. They aren’t perfect however and can be associated with false positives and negatives.
AN APPROACH TO THE WORKUP OF THESE PATIENTS
The Eastern Society for the Surgery of Trauma (11) in their approach to screening suspected BCI patients, did not consider isolated sternal fractures to predict BCI. They also proposed no further investigations in patients with a normal ECG and Troponin If all else was normal, the recommendation was for no monitoring of these patients.
IS THE ECG AN ADEQUATE SCREENING TOOL?
The ECG is often used as the initial screening tool in suspected BCI. It can however be normal in patients with significant BCI.
In one study(11) only 59% of patients with wall motion abnormalities or cardiac chamber dilatation on transoesophageal echocardiogram (TOE) had abnormal ECGs. Fukda et al(12) found that 41% of patients with a mechanism for BCI and an initial normal ECG developed clinically significant cardiac abnormalities. We therefor need to beware of false negatives. It is for this reason that I would perform a troponin at the same time.
TROPONIN AS A SCREENING TOOL?
The combination of ECG and high sensitivity troponin can be used to identify BCI. A raised troponin needs to be repeated, just as we would in a patient with acute coronary syndrome, keeping in mind that some BCI can also lead to ischaemia. If it normalises that may indicate that there is no need for monitoring.
We don’t know the best timing for repeating the troponin. However a cardiac strategy of 2-4 hours for a repeat test, is probably appropriate. We are also not quite sure of a threshold of troponin, where we should be concerned. Becker et al (13) in a recent retrospective study on the utility of high sensitivity troponin, found a HsTnI threshold of 40ng/L can be used as a threshold. We need to be aware that repeat the trauma itself can sometimes slightly raise the high sensitivity troponin.
AN APPROACH TO BCI
References
- Gao LM et al. Blunt cardiac injury: a single center 15 year experience. Am Surg 2020. 86:354-61
- El-Menyar A et al. Understanding traumatic blunt cardiac injury. Annals of Cardiac Anaesthesia 15(4):287-95
- Schultz JM, et al. Blunt cardiac injury. Crit Care Clin. 2004;20:57–70
- Gao JM, et al. Emergency surgery for blunt cardiac injury: experience in 43 cases. World J Surg. 2020;44:1666–1672.
- De Waele J et al. Blunt cardiac injury in patients with isolated sternal fractures: The importance of fracture grading. Eur J Trauma. 2002, 28:178-82.
- Athanassiadi K et al. Sternal fractures: retrospective analysis of 100 cases. World J Surg. 2002;28:1243-46
- Fokin AA et al. Blunt cardiac injury patients with sternal fractures. March 2022. Cureus 14(3):e22841
- Heidelberg L et al. The depth of sternal displacement is associated with blunt cardiac injury. Surg Res 2019:235:322-8
- Rashid M et al. Cardiovascular injuries associated with sternal fractures. Eur J Surg 2001;167:243-248
- Brookes JG et al. Sternal fracture:a retrospective analysis of 272 cases. J Trauma 1993,35:46-54
- Garcia-Fernandez M et al. Role of transesophageal echocardiography in assessment of patients with blunt chest trauma;correlation of echocardiographic finding with the electrocardiogram and creatinine kinase monoclonal antibody measurements. Am Heart J. 1998;135:476-81.
- Fukda G. An evaluation of serum troponin T and signal averaged electrocardiography in predicting electrocardiographic abnormalities after blunt chest trauma. J Trauma 1997;43:304-12.
- Becker E R et al. Re-evaluating the use of High Sensitivity Troponin to Diagnose Blunt Cardiac Injury. J Surg Res 2024 Aug:300:150-156.







