There is no optimal resuscitation strategy when dealing with septic shock. The management of fluids and vasoactive agents together with antibiotics is the cornerstone of treatment, however the optimal approach is uncertain. What is for certain is that this is a very heterogeneous group of patients and perhaps, just perhaps, as in cardiac resuscitation, a more tailored approach will provide improved survival.
The Study
Hernandez, Glenn et al. Personalized Hemodynamic Resuscitation Targeting Capillary Refill Time in Early Septic Shock-The ANDROMEDA-SHOCK-2 Randomized Clinical Trial. JAMA
What They Did
This was an investigator-generated, multicenter, randomized trial in patients ≥ 18years with early septic shock. They compared a tailored haemodynamic resuscitation protocol, which targetted capillary refill time to usual care. It involved 86 ICUs in 19 countries in the Americas, Europe, and Asia from 2022-2025.
Patients were recruited up to 4 hours after inclusion criteria were met and were randomised in a 1:1 ratio to Capillary Refill Time (CRT) protocol or usual care.
The study period was of 6 hour in duration, following recruitment.
N = 1467: 720 patients in the CRT intervention protocol and 747 patients to usual care.
Definition of Septic Shock/Inclusion Criteria:
- Suspected or confirmed infection, plus
- Hyperlactatemia (≥2.0 mmol/L), plus
- Requirement of norepinephrine(noradrenaline) following ≥ 1000mL if IV fluid to maintain a MAP of ≥ 65mmHg
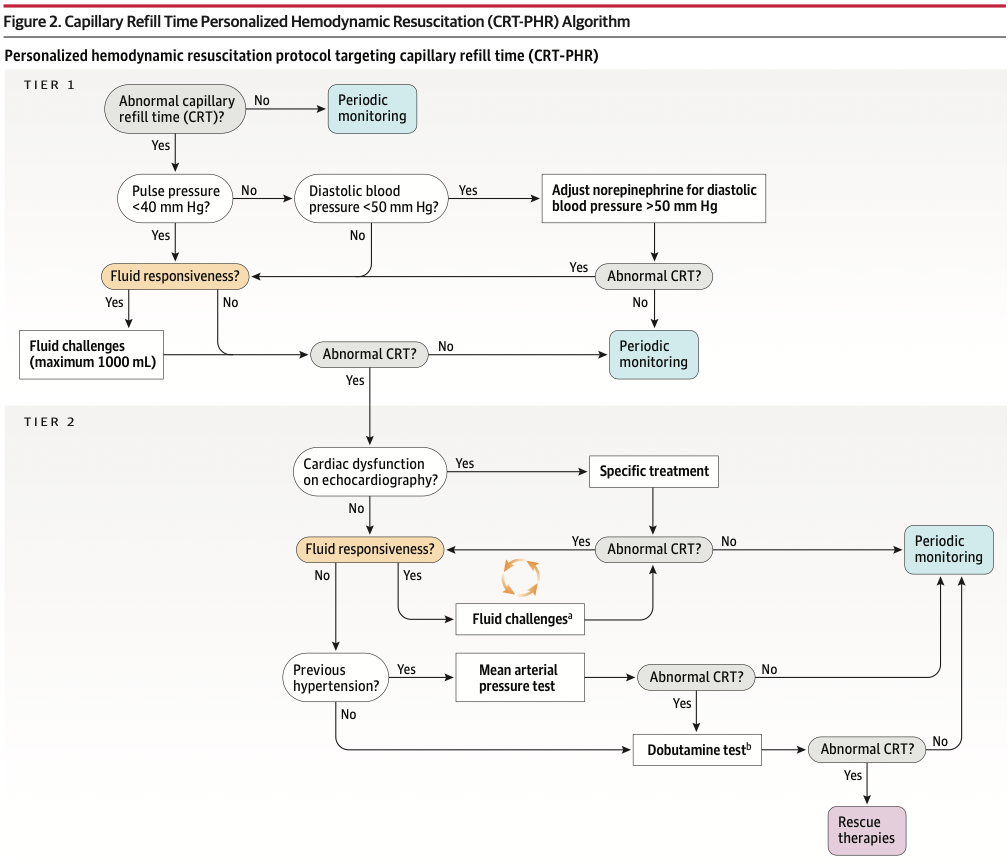
The CRT Algorithm included:
- CRT normalization as the target of hemodynamic resuscitation
- CRT was measured by applying pressure to the distal phalanx through a glass microscope slide, for 10 seconds, after the skin had blanched. Following release, the time to normal skin colour was timed.
- CRT > 3 seconds was considered abnormal.
- Identification of individual haemodynamic patterns of cardiovascular dysfunction including hypovolemia, vasoplegia, and cardiac dysfunction. These were assessed by pulse pressure(PP) and diastolic blood pressure(DBP) and basic bedside echocardiography
- Fluid-responsiveness assessment before any fluid resuscitation
- 2 hemodynamic tests:a trial of a higher Mean Arterial Pressure (MAP) target and a trial of fixed low-dose dobutamine.
The CRT algorithm approach to resuscitation had 2 tiers
Tier 1
If the CRT was normal, there was no further intervention, unless it became abnormal during monitoring. Almost 25% of the patients assigned to the CRT intervention had a normal CRT with no further treatment needed.
If the CRT was abnormal, then the PP and DBP was assessed.
Note:PP = SBP – DBP and is a measure of the force or pressure generated with each cardiac contraction. In this study, the PP was used as a surrogate marker of stroke volume. A PP of 40mm Hg or higher is considered normal. PP is determined by: stroke volume, total arterial compliance and arterial impedance. It increases with age due to changes in aortic impedance. A PP of <40 mm Hg indicates a low stroke volume that may be due to decreased preload of cardiac dysfunction.
- If the PP was low (< 40 mm Hg), then fluid responsiveness was assessed with a 500 mL fluid(colloid or crystalloid) fluid bolus. The CRT was then reassessed. A second bolus could be given (total maximum of 1000 mL of fluid). If the CRT normalised, then it was monitored. If the CRT continued to be abnormal, Tier 2 of the protocol was applied.
- If the PP was normal (> 40mm Hg) then the DBP was checked
- If DBP was < 50mm Hg the noradrenaline dose was increased to increase the DBP to > 50 mmHg. Following this, the CRT was checked: If normal, they continued to monitor, if abnormal, they gave a maximum of 1000 mL of fluid and checked responsiveness.
- If the DBP was > 50mm Hg fluid responsiveness was monitored
Note: DBP is mainly determined by vascular tone.
Tier 2
If the CRT was abnormal following Tier 1 of the algorithm, cardiac dysfunction was assessed on echocardiography.
Note: Left ventricular dysfunction has been traditionally measured by left ventricular ejection fraction, however fractional area change in the parasternal plane short axis, at the level of the papillary muscles correlates well with LVEF and has a prognostic value. Right ventricular systolic dysfunction can be assessed by right ventricular dilatation and a rise in central venous pressure.
- If Cardiac Dysfunction was present:
- If LV failure was present, there was an indication for Dobutamine. They gave specific treatment and reassessed CRT. If this was still abnormal they looked again at fluid responsiveness, with multiple fluid challenges as necessary.
- If there was RV failure present, further fluid resuscitation was ceased and a reduction in PEEP levels and ventilator plateau pressures was considered.
- If there was No Cardiac Dysfunction: They looked for further fluid responsiveness. If there was no response, they asked about previous history of hypertension.
- If there had been no previous hypertension, they started dobutamine at 5mcg/kg/min for one hour. if the CRT normalised this was maintained.
- If there had been previous hypertension then a Mean Arterial Pressure test was performed by increasing noradrenaline to a MAP of 80-85 mm Hg for one hour. If the CRT normalised the MAP was kept at this level for the 6 hours of the trial.
 Outcomes
Outcomes
Primary outcome: A hierarchical composite outcome:
- All-cause mortality within 28 days
- Duration of vital support including vasoactives,mechanical ventilation, kidney replacement therapy
- Length of hospital stay truncated at 28 days.
Secondary Outcomes: In hierarchical order:
-
All-cause mortality
-
Vital support–free days within 28 days of randomisation.
-
Length of hospital stay truncated at 28 days
The Patients
This was a sick group of patients.
- APACHE II scores of 14-24
- APACHE II estimates severity of disease and ICU mortality. It measures 12 physiologic variables at admission. Scores of 11-20 give a moderate risk of mortality, 21-30 have a high risk of mortality and above 31, a very high risk of mortality.
- SOFA scores of 7-11
- SOFA measures the severity of organ injury. The maximum score is 24. A score of 10 predicts 50% mortality
- Charlson Comorbidity Index of 2-5
- It is a score that predicts the risk of mortality in patients with multiple comorbidities. A score of 22 in. a patient with sepsis predicts an in-hospital mortality of 45%
What They Found
At 28 days following randomisation the number of ‘wins’ was greater in the CRT group 48.9% vs 42.1% is a6% difference, with duration of vital support yielding the highest number of wins. There was no significant difference in 28 day mortality between the two groups, although the CRT group had the higher number of organ support free days within 28 days and a faster decrease is SOFA .
Discussion
This is an unblinded study, with a complex protocol of escalating interventions, tailored to the ongoing clinical findings. The usual approach to septic shock management, is to target MAP and use fluids and pressors to obtain a MAP>65. The simplicity of using CRT instead of MAP, has been promoted as being more effective for resource poor areas, may be partly negated by the need for early echocardiography in Tier 2 of this protocol. That being said, most patients did achieve CRT normalisation with Tier 1 interventions in this study.
The lack of statistically significant mortality findings in this study, do not make it less important. It introduces important concepts of how we might tailor resuscitation by understanding and using parameters of PP and DBP to determine the interventions we use.
The approach of using the CRT to assess perfusion, makes perfect sense. If the CRT is low, we need to decide if this is a pump, pipes or filling problem. The reproducibility of CRT and the factors that may affect it, may be questioned. It is not as definitive as a MAP number and variations in technique and the operator-dependant nature of the procedure may affect the results.
The PP used as a surrogate marker for stroke volume, can be used to tailor treatment. A low PP (< 40mm Hg), requires us to seek the cause, being either pump, pipes or filling, or a combination of these. Fluid challenges can be tailored and used if there is no right cardiac dysfunction. Ventilator settings can be changed if there is.
A normal PP (> 40 mm Hg) but prolonged CRT, is a signal for a fluid challenge or pressor use. The DBP can guide our decisions.
- A low DBP can reflect vasodilatation (as long as the aortic valve is not damaged) and can decrease coronary perfusion, resulting in ischaemia and a decrease in stroke volume, resulting in a higher rate of cardiovascular events and mortality. Noradrenaline can be used to reverse vasoplegia.
- A normal DBP may be a signal for a fluid challenge.
This type of tailored thinking is important when dealing with complex septic patients.







